





Abstract
In the present case report, we have described the incidental finding of a gastrointestinal stromal tumor (GIST) in the appendix following surgical evaluation of a possible closed loop small bowel obstruction in the right lower quadrant. Upon exploration inside the abdomen, the distal ileum and proximal cecum appeared dusky with chronic strictures. An ileocecectomy was performed, and pathology returned with an incidental GIST of the appendix with a T1N0 classification.
Introduction
A gastrointestinal stromal tumor (GIST) is a rare tumor known as a sarcoma derived from the interstitial cells of Cajal (ICCs) and their precursor neural crest cells [1]. ICCs function as pacemakers of the gastrointestinal tract and assist in neural transmission [2]. GISTs account for fewer than 1% of gastrointestinal tumors [3]. GISTs can arise anywhere in the gastrointestinal tract, however around 50% of the time they arise in the stomach. The next most common site is the small intestine followed by the colon, rectum, and esophagus [4]. GISTs found in the appendix are exceedingly rare, accounting for 0.1%–0.2% of all GISTs [3].
A GIST is usually diagnosed with immunohistochemistry for the expression of KIT protein (CD117), a receptor tyrosine kinase protein [1]. Discoveries have shown that GISTs have numerous genetic alterations. These alterations help dictate the path of treatment [5]. The following case presents a patient who had an incidental finding of a GIST in her appendix.
Case report
We present a case with an 88-year-old patient with a history of dementia, hypertension, hypothyroidism, diabetes mellitus, chronic obstructive pulmonary disease, and stage 3b chronic kidney disease who presented to the emergency department from her nursing home with worsening diffuse abdominal pain. Due to her dementia, she was a poor historian and was unable to remember when her last bowel movement was. Per nursing home records, it was suggested that she had a three-day history of nausea and vomiting. The pertinent initial laboratory test results, history details, and imaging results are presented in Table 1.
Patient demographics, medical history, and operative details.
| Variable | Details |
|---|---|
| Admission data and patient demographics | |
| Age | 88 |
| Gender | Female |
| Medical History | Insulin dependent type II DM, HTN, CKD stage IIIB, dementia |
| Symptoms upon arrival | Nausea, vomiting, abdominal pain all over, abdominal distension |
| Vital Signs in Emergency Department | |
| Temperature Pulse Rate Respiratory Rate Blood Pressure | 98.3 83 17 170/82 |
| Pertinent admission laboratory test results | |
| Sodium Potassium Lactic Acid BUN Creatinine RBC Hgb Hct Platelet Count WBC ANC | 136 4.1 2.3 37 1.42 5.6 16.0 51.6% 166 8.4 6.45 |
| Surgical history | None |
| Admission imaging studies | CT A&P: Dilated loops of small bowel with air-fluid levels. Two transition points in RLQ with potentially closed loop component to the extensive small bowel obstruction. Additionally, large hiatal hernia. |
| Surgery | |
| Procedure | Exploratory laparotomy, ileocectomy |
| Hospital day performed | 1 |
| Operative time | 80 minutes |
| EBL | 10 mL |
| Intraoperative transfusions | 5% albumin 500 ml |
| Postoperative details | Developed ileus, return of bowel function on POD 5 |
| Overall length of stay | 18 days |
| Discharge Disposition | Skilled Nursing Facility |
CT abdomen and pelvis scan demonstrated dilated loops of small bowel with a likely closed-loop component as seen in Fig. 1. Imaging also showed a large hiatal hernia with significant gastric distension. Surgery was consulted and the patient was taken to the operating room expeditiously.
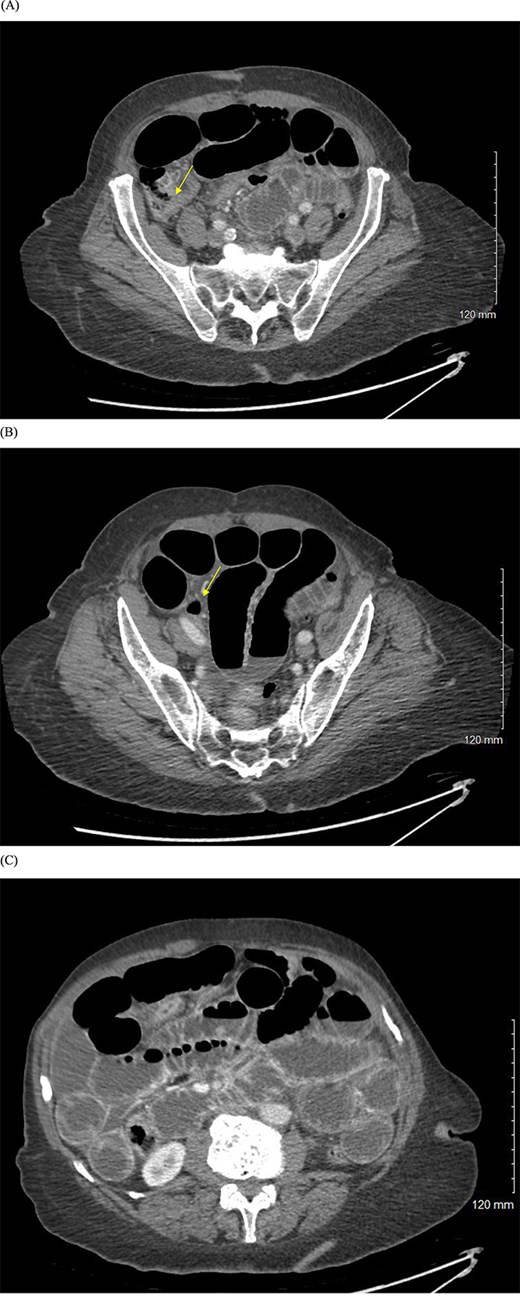
(A, B) CT abdomen and pelvis with IV contrast showing evidence of small bowel obstruction with two transition points in the right lower quadrant (yellow arrows). (C) Dilated loops of small bowel with air-fluid levels.
In the operating room, a midline laparotomy was performed. After entering the abdomen, a single band causing the closed loop obstruction in the distal ileum was identified and divided. The ileum involved within the closed loop obstruction, as well as proximal cecum, appeared dusky. Associated mesentery in this area had significant ecchymosis and chronic strictures were noted at the ileocecal valve. Due to the proximity of the ileocecal valve to the strictures and dusky color of the area, a decision was made to perform an ileocectomy. Following resection with ileocolic anastomosis, the small bowel was run in its entirety with no additional concerns and no evidence of carcinomatosis or obvious lesions in the small bowel. The abdomen was irrigated and closed. The specimen of ileum with cuff of cecum and appendix were sent to pathology for evaluation.
Final pathology report of the cecum, appendix, and terminal ileum following the ileocectomy verified an incidental GIST in the appendix. The GIST’s final staging was pT1 N0. Tumor cells were positive for CD34, KIT (CD117), and DOG1, while negative for pancytokeratin, desmin, S100, and SMA supporting the findings. Benign small bowel and colonic tissue serosal adhesions were also noted along with three benign mesenteric lymph nodes.
The patient’s hospital course was marked with expected postoperative ileus development with eventual return of bowel function on post-op Day 5. By post-op Day 10, plans for discharge were aborted due to an acute rise in leukocytosis. CT scan revealed a large pelvic abscess which was subsequently drained by interventional radiology. Drain output was consistent with old, infected hematoma. She was started on broad spectrum antibiotics, and over the course of several days, her leukocytosis resolved. On POD 18, she was ultimately discharged to a skilled nursing facility. Due to the low grade nature of the GIST, no further oncologic treatment was deemed necessary.
Discussion
The patient presented in this case had concern for a closed component obstruction, for which she was taken to the operating room where an exploratory laparotomy and ileocectomy was performed. Final pathology of the specimen revealed a GIST in the appendix. GISTs found in the appendix are exceptionally rare, representing only 0.1% of cases [6]. The number of cases in literature confirming the finding of GISTs in the appendix are very minimal with only 20 reported cases [7]. Some documented cases of incidental GIST discoveries in the appendix presented with appendicitis-like symptoms without pathologic evidence of appendicitis, which suggests that the tumor was the cause of the symptoms [8]. The rest of the documented GISTs in the appendix were found incidentally during surgery or at autopsy [9].
GISTs have a wide range of clinical possibilities from virtually no metastatic possibility to life threatening malignant disease. When a GIST is found, complete surgical resection is the standard of curative treatment [10]. Next, risk stratification is performed, which includes tumor size, mitotic rate, origin site, margin status, and molecular mutation [11]. When risk of recurrence is high and the tumor indicates a tyrosine kinase inhibitor sensitive mutation is present, a tyrosine kinase inhibitor, usually imatinib, is indicated for adjuvant therapy. For low risk or very low risk GISTs that are incidentally found following resection, like in the presented case, no follow up or annual CT scan is appropriate [10].
Acknowledgements
The author would like to thank Grandview Medical Center for providing its help and resources to make this report possible.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}