





Abstract
Rectal diverticulum is an exceedingly rare clinical entity, typically occurring as a solitary lesion or, less frequently, as up to three diverticula. Its development is often associated with underlying conditions such as obstructive defecation syndrome, rectal malignancy, pelvic floor weakness, chronic rectal impaction, obesity, or infection-related muscular atrophy. Although uncommon, rectal diverticulitis represents a surgical emergency requiring timely recognition and management. In this case, a female patient presented with rectal bleeding and secondary anemia. During the clinical course, the patient developed pelvic sepsis secondary to rectal diverticulitis. Appropriate surgical intervention, combined with antimicrobial therapy and supportive management, led to a favorable outcome. Rectal diverticulitis is a rare but potentially life-threatening condition. Awareness of this entity and early diagnosis are essential to prevent severe complications such as perforation and pelvic sepsis. This case highlights the importance of considering rectal diverticulum in the differential diagnosis of lower gastrointestinal bleeding and pelvic infections.
Introduction
Despite the high frequency of diverticulosis of the colon, especially in the sigmoid, rectal diverticulosis has been rarely described and reported. Its incidence is estimated to be less than 0.1%. Unlike colonic diverticula, rectal diverticula are true diverticula that include all layers of the bowel wall. They tend to be larger, have a wider opening, and occur less frequently [1 to 3]. These diverticula are mostly asymptomatic but can present with hematochezia, secondary anemia, abdominal and rectal pain, tenesmus, rectal stenosis, and various types of fistulas between the rectum and other pelvic organs [1, 2]. In case of diverticular perforation, abscess formation, or pelvic sepsis may occur, requiring prompt diagnosis and appropriate treatment [1]. This is a report of a perforated solitary mid-rectal diverticulum presenting with secondary anemia and hematochezia, followed by pelvic sepsis. Written informed consent was obtained from the patient’s son.
Case report
An 84-year-old female patient presented with massive hematochezia without a physiologic bowel movement that day. Previous comorbidities reported were hypertension and diabetes mellitus. Two months ago, the patient reported being treated with blood units due to unexplained anemia, with no further diagnostics conducted. On admission, the abdominal physical exam was unremarkable. The digital rectal exam revealed blood in the rectum. The laboratory test revealed a low erythrocyte count of 2.36 × 106/μL (3.93–6.08), Hemoglobin level of 7.8 g/dL (11/2–17.5), Hematocrit % of 24.3 (34.1–51), Leucocyte count of 18.1 × 103/μL, Neutrophil % of 85.7 (34–71.1), serum glucose level of 24.5 mmol/L (3.3–5.6), and albumin level of 33 g/L (34–50). The patient was admitted for resuscitation and further investigation. Two units of blood were given. A diagnostic colonoscopy performed the next day revealed sigmoid diverticulosis and a solitary mid-rectal diverticulum with a wide opening and necrotic bottom (Fig. 1). The patient presented with two episodes of fever, reaching a maximum of 38.3°C. On the third day of admission, an elevated level of procalcitonin (27 ng/mL), (0.05–0.1), Leukocytosis of 23.0 × 103/μL, and a CRP level of 248 mg/L (0–5) were noted. The general condition of the patient slightly worsened, and the repeated abdominal physical exam remained unremarkable. A contrast-enhanced abdominal computerized tomography showed free air around the mid rectum in the pelvis (Fig. 2) with cranial retroperitoneal extension (Fig. 3). Emergency laparotomy was indicated. No signs of peritonitis were noted. After rectal mobilization and dissecting distally, a gas bubble occurred. Further distal dissection revealed a small abscess on the anterolateral wall with a visible opening in the rectal wall. A low Hartmann procedure was performed (Fig. 4). The postoperative period was uneventful. The length of hospital stay was 9 days. Pathology analysis confirmed the presence of a solitary rectal diverticulum perforation with accompanying diverticulitis.

The colonoscopy finding shows a rectal diverticulum with a necrotic bottom.
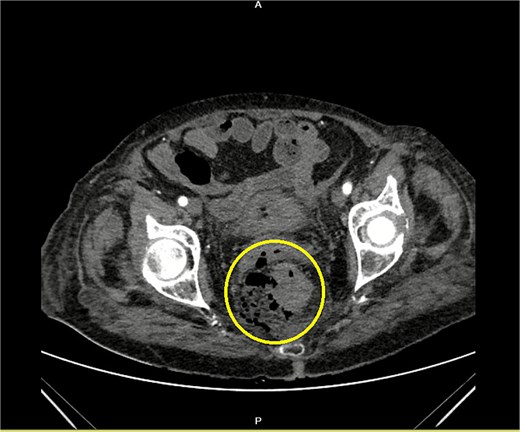
Contrast-enhanced CT of the pelvis showing free air around the rectum with a visible defect of the rectal wall (encircled).
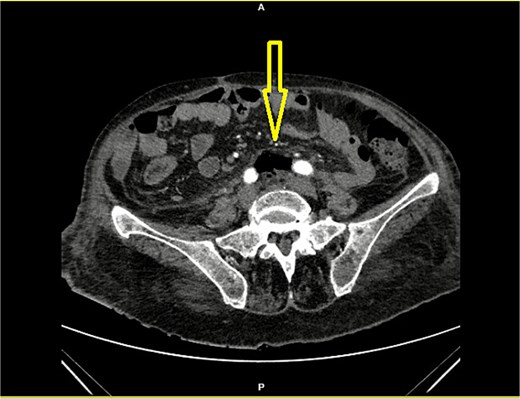
Contrast-enhanced CT of the abdomen showing retroperitoneal air (arrow) below the aortic bifurcation (between the common iliac arteries).
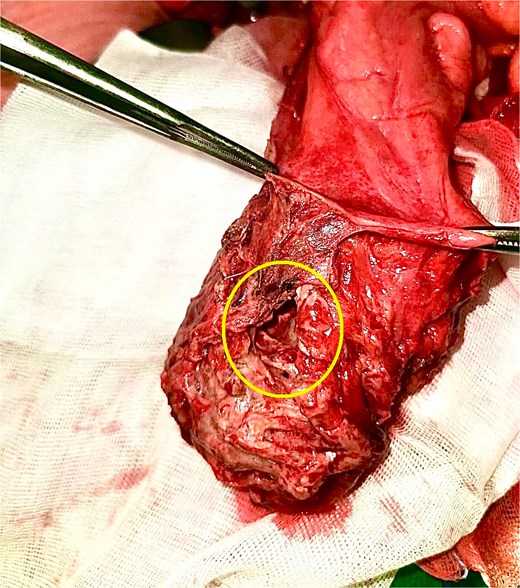
Operative specimen with free extraperitoneal rectal perforation (instruments holding the peritoneal reflection).
Discussion
Rectal diverticulosis is a rare condition with a reported range of incidence between 0.07 and 0.4% [3]. Its rarity, contrary to the sigmoid colon, is reported to be explained by the anatomical presence of continuous longitudinal and circular muscle fibers of the rectum, its decreased peristaltic activity, and the decreased intraluminal rectal pressure. Factors reported to be responsible for or influencing rectal diverticula formation are the congenital ones, chronic constipation (obstructed defecation syndrome), repetitive rectal impaction, pelvic floor muscle weakness, obesity, and infection-related muscle atrophy [1–4]. Cases of rectal cancer within the diverticulum have been reported [5]. In the past decade, a post-procedural iatrogenic rectal and pelvic weakness has been described as a predisposing factor for diverticula, such as stapled haemorrhoidopexy, and stapled transanal rectal resection procedure for obstructed defecation [1, 6].
Most of the rectal diverticula are asymptomatic. However, symptoms are present in some patients, such as abdominal and pelvic pain, hematochezia, tenesmus, and purulent discharge. Furthermore, fecal impaction of the diverticulum may lead to rectal diverticulitis, which can result in subsequent perforation, abscess formation, or pelvic sepsis [2, 7, 8].
Cases of rectal diverticulitis necessitating emergency treatment are rare, with only a few published (Table 1). The treatment options in such cases include antibiotic use, radiologic drainage, interventional endoscopy, and surgery [1].
Published cases of complicated rectal diverticula treated with surgery in emergency settings
| Reference | Author/year | Patient age/gender | Physical findings and laboratory abnormalities | Diagnosis establishment tool | Location of perforation | Treatment |
|---|---|---|---|---|---|---|
| [9] | Takeuchi et al./2009 | 62/F | Acute abdomen, tachycardia, fever, leukocytosis, elevated CRP | CT scan | Upper rectum | Hartmann’s procedure |
| [8] | Özçelik et al./2015 | 63/F | Abdominal pain, nausea, vomiting | CT scan, rectal contrast transition | Upper rectum | Hysterectomy, right salpingo-oophorectomy, Hartmann’s procedure |
| [7] | Gorgoraptis et al./2020 | 49/F | Lower abdominal pain, weakness, paraparesis, leukocytosis, impaired renal function | Ultrasound, CT scan, MRI | Extra peritoneal rectum | Loop colostomy, with lavage and drain |
| [2] | Tulenko et al./2025 | 42/F | Abdominal tenderness, leukocytosis, hematochezia | CT scan, MRI, sigmoidoscopy | Extra peritoneal rectum | Proctectomy with bilateral ureteral stent placement, hysterectomy with bilateral salpingectomy, and posterior vaginal wall repair |
| This report | Nikolovski et al./2026 | 84/F | Weakness, leukocytosis, hematochezia, anemia, fever, elevated CRP, and procalcitonin | Colonoscopy, CT scan | Middle rectum | Low Hartmann’s procedure |
The range of diagnostic methods for detecting rectal diverticula includes computed tomography (CT) scans with rectal contrast, magnetic resonance imaging (MRI), barium enema, and flexible colonoscopies [2, 10, 11]. In emergency cases of suspected rectal diverticulitis and/or rectal diverticulum perforation, a pelvic CT scan will reveal local inflammation with extraluminal air leak, as in this case.
Asymptomatic rectal diverticula need no treatment. The ones that cause symptoms should be treated. The treatment should be individualized due to the underlying cause of the diverticulum. Cases with rectal cancer need to be approached with oncologic principles. In patients with obstructive defecation, rectal resection/proctectomy or mesh rectopexy are the options [2, 4, 12]. In other cases, transanal diverticulectomy is the choice [6, 13]. Recently, a new method of transanal minimally invasive surgery was introduced for transanal diverticulectomy [14]. Cases of uncomplicated diverticulitis can be initially treated with intravenous antibiotics. If a complicated diverticulitis is encountered, radiologic and surgical drainage, diverting stoma, and Hartmann’s procedure are the options [1].
Conclusion
Rectal diverticula are exceedingly uncommon, and their presentation with complications such as hemorrhage or diverticulitis is exceptionally rare. This report is about a unique case of an inflamed mid-rectal diverticulum complicated by bleeding and perforation, subsequently leading to pelvic sepsis. Prompt surgical intervention resulted in complete resolution of the sepsis and a favorable postoperative outcome. This case underscores the importance of considering rectal diverticular disease in the differential diagnosis of lower gastrointestinal complications, particularly in atypical clinical presentations such as bleeding per rectum.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}