





Abstract
Accidental ingestion of fish bones is common, but gastrointestinal perforation remains an uncommon complication (<1%). We report the case of a 35-year-old man who developed one week of abdominal pain after consuming a seafood meal. Contrast-enhanced computed tomography demonstrated a radiopaque linear structure measuring approximately 3 cm penetrating a jejunal loop into the mesenteric fat, with associated fat stranding. Diagnostic laparoscopy identified a fish bone perforating the jejunum; the foreign body was removed, and the bowel defect was closed primarily. The postoperative recovery was uncomplicated. A literature review from 2014 to 2025 identified ten comparable cases of fish-bone-related small bowel perforation. These cases highlight diagnostic challenges due to non-specific symptoms and variable imaging findings. Prompt CT imaging and early minimally invasive surgical intervention improve outcomes. Fish-bone perforation should remain part of the differential diagnosis in patients with unexplained abdominal pain following seafood ingestion.
Introduction
Accidental ingestion of fish bones is relatively common; however, gastrointestinal perforation is rare, occurring in fewer than 1% of cases [1]. Clinical presentation is often vague, making diagnosis challenging. Many patients do not recall ingesting a foreign body, and early symptoms may be mild or subacute. Computed tomography (CT) is the most sensitive imaging modality for detecting fish bones, allowing visualization of linear hyperdense objects, bowel wall breach, and localized inflammatory changes [1, 2].
This report describes a case of jejunal perforation caused by a fish bone penetrating into the mesenteric fat, successfully treated with laparoscopic removal and primary repair. A review of previously published cases is also presented to emphasize diagnostic pitfalls and optimal management strategies.
Case presentation
A 35-year-old previously healthy male presented with a one-week history of intermittent, dull periumbilical abdominal pain that began after eating a seafood meal. He denied fever, vomiting, gastrointestinal bleeding, or altered bowel habits and did not recall swallowing a fish bone.
On presentation, vital signs were within normal limits. Abdominal examination revealed focal periumbilical tenderness without guarding or rigidity. Laboratory investigations demonstrated mild leukocytosis and an elevated C-reactive protein level.
Contrast-enhanced CT of the abdomen revealed a radiopaque linear foreign body measuring approximately 3 cm lodged within a jejunal loop, penetrating the bowel wall into the adjacent mesenteric fat. Prominent fat stranding was present, without evidence of free intraperitoneal air, bowel obstruction, or abscess formation (Fig. 1).

Contrast-enhanced CT scan showing ~3 cm radiopaque linear foreign body lodged within a jejunal loop, penetrating the bowel wall into adjacent mesenteric fat.
Previous case reports of fish bone gastrointestinal perforation (2021–2025) (1–12)
| Author & year | Age / sex | Location of perforation | Imaging findings | Management | Outcome | Reference |
|---|---|---|---|---|---|---|
| Choi et al., 2014 | 54 M | Jejunum | Linear hyperdense FB, fat stranding | Laparoscopic removal + primary repair | Recovered | [3] |
| Husain et al., 2022 | 45 F | Distal ileum | Radiopaque FB, local inflammation | Laparotomy + resection | Recovered | [4] |
| Santos et al., 2019 | 39 M | Proximal jejunum | Hyperdense linear FB | Laparoscopic extraction + repair | Recovered | [5] |
| Nakahara et al., 2025 | 72 F | Jejunum (mesenteric penetration) | FB embedded in mesentery | Laparoscopic removal | Recovered | [6] |
| Yuki et al., 2012 | 58 M | Ileum | Calcified FB + focal fluid | Laparoscopic extraction + repair | Recovered | [7] |
| Parakh and Abujudeh, 2021 | 62 F | Small bowel (unspecified) | CT difficult due to angulation | Exploratory laparoscopy | Recovered | [8] |
| Jallali et al., 2024 | 33 M | Ileum | Hyperdense FB + fat stranding | Laparoscopy + primary closure | Recovered | [9] |
| Al Hosein and Eghtedari, 2023 | 48 M | Mid-ileum | Focal perforation | Laparotomy + resection | Recovered | [10] |
| Yamaguchi, 2023 | 66 F | Jejunum | Hyperdense linear FB | Laparoscopic removal | Recovered | [11] |
| Li et al., 2025 | 59 F | Gastric + gallbladder injury | Multiorgan penetration | Surgical removal + repair | Recovered | [12] |
Based on these findings, diagnostic laparoscopy was performed.
Intraoperative technique
A standard three-port laparoscopic approach was utilized. After pneumoperitoneum was established via an umbilical port, a 10-mm camera port and two 5-mm working ports were inserted under direct visualization. Systematic inspection of the small bowel identified an inflamed jejunal segment approximately 120 cm distal to the ligament of Treitz.
A sharp foreign body, later confirmed to be a fish bone measuring approximately 3 cm, was observed protruding through the antimesenteric border of the jejunum into the mesenteric fat. Gentle blunt and sharp dissection was performed to release surrounding adhesions, allowing safe extraction of the foreign body (Fig. 2).
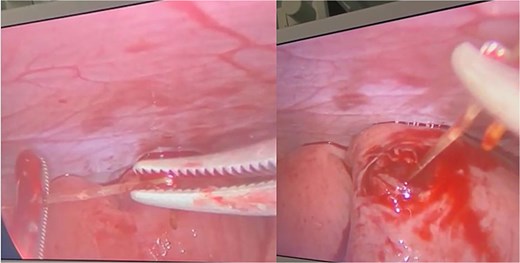
Intraoperative laparoscopic view demonstrating a sharp foreign body—later confirmed as a ~3 cm fish bone—was seen protruding through the antimesenteric border into the mesenteric fat.
The perforation site, measuring approximately 4–5 mm, was minimally debrided and closed primarily in two layers. The inner layer consisted of interrupted 3–0 absorbable sutures approximating the mucosa and submucosa, followed by an outer layer of Lembert seromuscular sutures for reinforcement. The integrity of the repair was tested using saline insufflation. The abdominal cavity was irrigated, and a small suction drain was placed.
Postoperative course
The patient recovered uneventfully, resumed oral intake gradually, and was discharged in stable condition. At four-week follow-up, he remained asymptomatic.
Discussion
Fish bone perforation of the gastrointestinal tract presents a diagnostic challenge due to its rarity and non-specific clinical presentation. Many patients do not recall foreign body ingestion, and symptoms may be mild or subacute, leading to delays in diagnosis [1, 3]. Computed tomography plays a crucial role in detection, as it can identify linear hyperdense foreign bodies as well as secondary signs such as localized bowel wall thickening and surrounding mesenteric fat stranding, which are among the most reliable indicators of sharp foreign body perforation [1, 2].
Although ileal perforation is reported more frequently, jejunal perforation is well documented in the literature. Several recent case reports describe fish bones embedded within the mesentery, producing localized inflammatory reactions similar to the findings observed in the present case [3–7]. Management strategies vary depending on the extent of contamination and bowel injury, ranging from laparoscopic extraction with primary repair to segmental bowel resection in cases complicated by abscess formation or devitalized bowel.
In haemodynamically stable patients without diffuse peritonitis, laparoscopic management is preferred. The minimally invasive approach provides excellent visualization, reduced postoperative pain, shorter hospital stay, and favorable clinical outcomes. Segmental bowel resection should be reserved for cases with friable tissue, necrosis, or extensive contamination.
Fish bones are thin and variably calcified and may align parallel to CT planes, making them difficult to detect. Therefore, secondary CT findings such as focal mesenteric inflammation, fat stranding, and localized bowel wall thickening should raise suspicion for foreign body perforation [8, 9]. When diagnosis is established early, prognosis is excellent. Delayed recognition increases the risk of abscess formation, peritonitis, sepsis, and fistula development [1]. The favorable outcome in this case underscores the importance of prompt imaging and early minimally invasive surgical intervention [10, 11].
Learning points
Fish-bone perforation should be considered in patients with unexplained abdominal pain following seafood ingestion, even when ingestion is not recalled.
CT imaging is the diagnostic modality of choice; linear hyperdensity with adjacent fat stranding is highly suggestive.
Laparoscopic extraction with primary repair is safe and effective in stable patients.
Early diagnosis prevents serious complications, including abscess formation, peritonitis, and fistula development.
Postoperative follow-up is essential to ensure complete healing.
Conclusion
This case highlights a rare but clinically important cause of abdominal pain: jejunal perforation by a fish bone penetrating into the mesenteric fat. Prompt CT diagnosis and laparoscopic management resulted in an excellent outcome. Clinicians should maintain a high index of suspicion when evaluating patients with subacute abdominal pain following fish consumption [12].
Conflicts of interest
None declared.
Funding
None declared.
References
Yuki T, Ishihara S, Okada M et al.
Parakh A, Abujudeh HH.

{kind=link}
{kind=link}