





Abstract
Schistosomiasis is a neglected tropical disease with significant morbidity, yet appendicitis secondary to schistosomal infestation remains rare, even in endemic regions. We report a series of five cases of acute appendicitis in adult patients, where histopathological examination revealed schistosomal appendicitis. All patients presented with classical features of acute appendicitis, underwent appendectomy, and recovered uneventfully. One case demonstrated mural calcifications on preoperative imaging, raising suspicion of schistosomiasis preoperatively. Histology confirmed the diagnosis in all cases. This report highlights the importance of routine histopathological examination of appendectomy specimens in endemic areas, as schistosomiasis may mimic common surgical emergencies and requires targeted antiparasitic treatment postoperatively to prevent further complications.
Introduction
Human schistosomiasis is a neglected tropical disease caused by Schistosoma species and occurs mainly in tropical and subtropical countries [1]. It is a parasitic infection induced by different species, either intestinal (Schistosoma mansoni, S. japonicum, S. mekongi, S. guineensis, S. intercalatum) or urogenital (S. haematobium) [1]. The disease predominantly affects rural and poor communities, especially agricultural and fishing populations [2]. Globally, schistosomiasis accounts for an estimated burden of 1.4 million disability-adjusted life years [1].
The infection is endemic in the Eastern Mediterranean, sub-Saharan Africa, the Arab Peninsula, and parts of the Indian Ocean [2]. Turner first described appendicular schistosomiasis in 1909 [3]. In Saudi Arabia, a high prevalence of schistosomiasis has been reported [4]. In one retrospective study from Abha, Saudi Arabia, 4708 appendices were reviewed, and schistosomal appendicitis (SA) was found in 64 (1.35%) specimens [5]. Appendicitis may be the first clinical manifestation of underlying schistosomiasis, necessitating specific antiparasitic treatment [5].
Case presentations
Case 1
A 31-year-old male, previously healthy, presented with a 1-day history of right lower quadrant pain, associated with nausea, vomiting, anorexia, and fever. Examination revealed right iliac fossa tenderness and rebound tenderness. Laboratory tests showed a white blood cell (WBC) count of 6–10 × 109/l. Abdominal computed tomography (CT) was suggestive of acute appendicitis with early gangrenous changes. The patient underwent laparoscopic appendectomy. Intraoperative findings included an appendicular mucocele. Recovery was uneventful, and he was discharged on postoperative day 1.
Final histopathological examination revealed the appendix shows diffuse mucosal and focally transmural granulomatous inflammation surrounding Bilharizial ova (Fig. 1a and b).
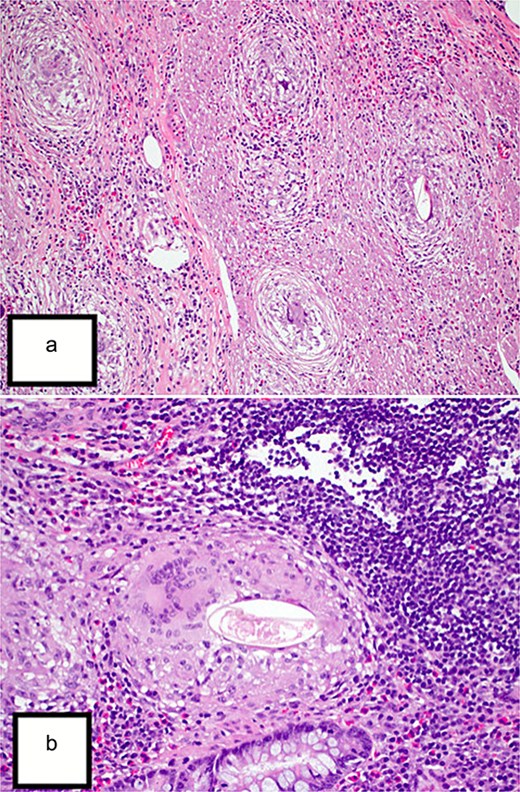
(a) Hematoxylin and eosin (H&E) stain (10×) revealed the appendix shows diffuse mucosal and focally transmural granulomatous inflammation surrounding Bilharizial ova. (b) H&E stain (40×) revealed the appendix shows diffuse mucosal and focally transmural granulomatous inflammation surrounding Bilharizial ova.
Summary of the five cases of schistosomal appendicitis this table highlights the key demographic, clinical, radiological, operative, and outcome data across all five patients.
| Age/sex | Presentation | Imaging | Intraoperative findings | Outcome |
|---|---|---|---|---|
| 31/M | 1-Day history of RLQ pain, nausea, vomiting, fever | CT: early gangrenous appendicitis | Appendicular mucocele | Laparoscopic appendectomy; discharged day 1 |
| 35/M (Egyptian) | 12 h periumbilical pain → RLQ, chills | CT: acute appendicitis | Inflamed appendix, healthy base, no perforation | Open appendectomy; discharged day 2 on antibiotics |
| 45/F | RLQ pain, vomiting, no fever/diarrhea | CT: early acute appendicitis | Inflamed, non-perforated appendix | Open appendectomy; discharged day 2 |
| 36/F (housemaid) | 2-Day supraumbilical pain → RLQ, nausea, vomiting | CT: perforated appendicitis with mural calcifications (suggestive of schistosomiasis) | Inflamed, perforated appendix | Open appendectomy; discharged day 5 |
| 36/M | Colicky abdominal pain, vomiting, fever 38°C | CT: uncomplicated appendicitis | Inflamed, non-gangrenous appendix | Open appendectomy; discharged day 1 |
Case 2
A 35-year-old Egyptian male presented with 12 h of periumbilical pain shifting to the right lower quadrant, associated with chills. There were no systemic symptoms. Examination showed localized tenderness without rebound. WBC count was 14.6 × 109/l. CT abdomen suggested acute appendicitis. An open appendectomy revealed an inflamed appendix with healthy base and no perforation. The patient recovered well and was discharged on postoperative day 2 with antibiotics.
Final histopathological examination revealed the appendix show focal submucosal deposition of Bilharizial ova with focal granulomatous inflammation (Fig. 2).
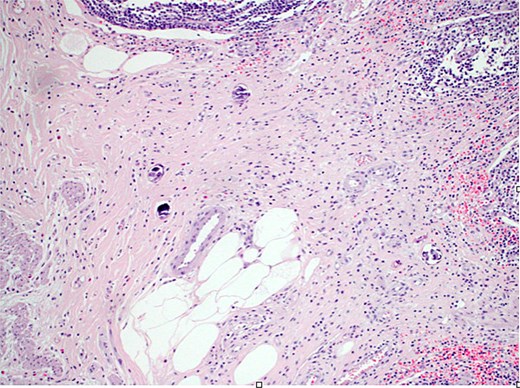
H&E stain (10×) revealed the appendix shows focal submucosal deposition of Bilharizial ova with focal granulomatous inflammation.
Case 3
A 45-year-old female presented with 1 day of right lower quadrant pain and two episodes of vomiting. There was no fever, diarrhea, or constipation. Examination showed right lower quadrant tenderness without rebound. WBC was 10.3 × 109/l. CT abdomen suggested early acute appendicitis. Open appendectomy revealed an inflamed, non-perforated appendix. She recovered well and was discharged on postoperative day 2.
Final histopathological examination revealed the appendix show extensive transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis (Fig. 3a and b).
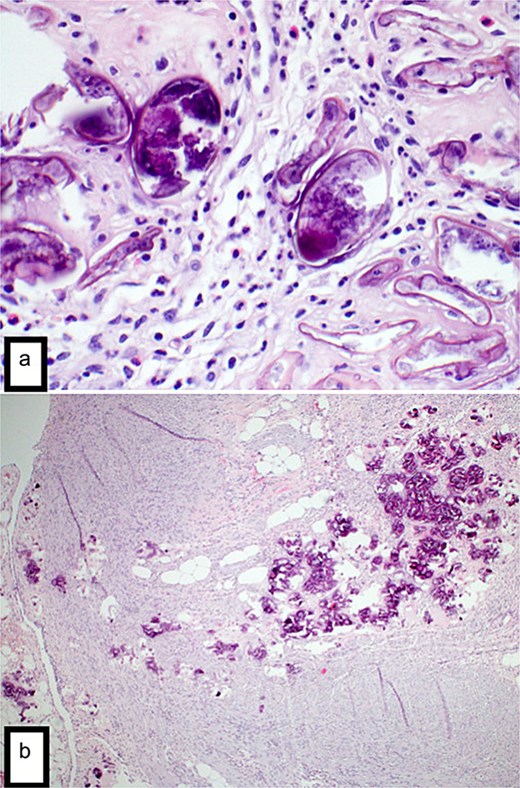
(a) H&E stain (4×) revealed the appendix shows focal transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis. (b) H&E stain (40×) revealed the appendix shows focal transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis.
Case 4
A 36-year-old female housemaid presented with 2 days of abdominal pain, initially supraumbilical then localizing to the right iliac fossa, associated with nausea and vomiting. Examination showed localized tenderness with rebound. WBC was 11.6 × 109/l. CT revealed acute perforated appendicitis with mural calcifications extending to the cecum and ascending colon, with a differential diagnosis of schistosomiasis or mucocele. Open appendectomy was performed. The postoperative course was uneventful, and she was discharged on day 5.
Final histopathological examination revealed the appendix shows focal transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis (Fig. 4a and b).
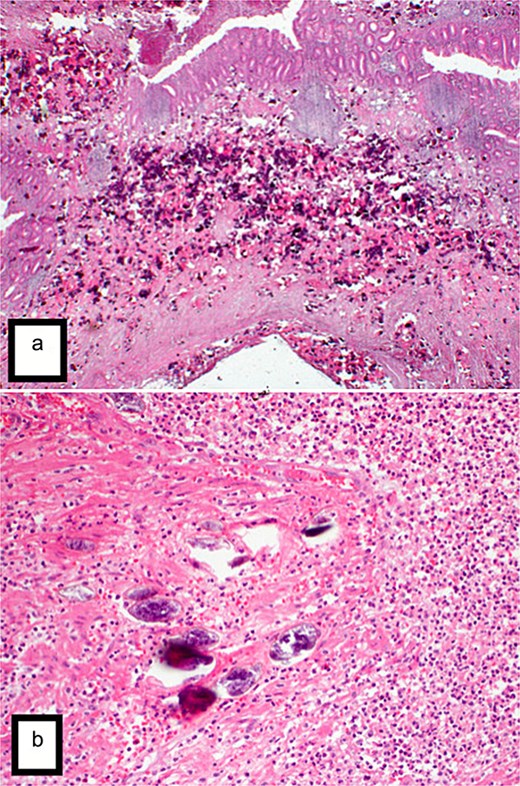
(a) H&E stain (2×) revealed the appendix shows extensive transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis. (b) H&E stain (20×) revealed the appendix shows extensive transmural deposition of calcified Bilharizial ova on the background of acute suppurative appendicitis with periappendicitis.
Case 5
A 36-year-old male presented with colicky abdominal pain shifting from periumbilical to right lower quadrant, associated with three episodes of vomiting and anorexia. He was febrile (38°C). WBC was 10.6 × 109/l. CT abdomen showed acute uncomplicated appendicitis. Open appendectomy revealed an inflamed, non-gangrenous appendix. He was discharged in good condition on postoperative day 1.
Final histopathological examination revealed the appendix show focal submucosal deposition of Bilharizial ova with focal granulomatous inflammation (Fig. 5a).
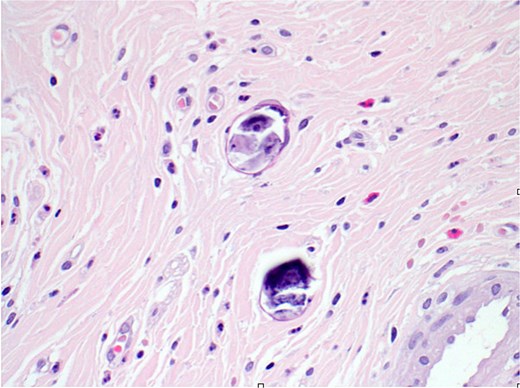
H&E stain (40×) revealed the appendix shows focal submucosal deposition of Bilharizial ova with focal granulomatous inflammation.
Discussion
Appendicitis is the most common abdominal surgical emergency worldwide [6]. Its etiology is multifactorial, with luminal obstruction considered the main hypothesis [6]. Parasitic infestation is an uncommon cause, representing 5.3% of appendectomy specimens in some studies, with schistosomiasis accounting for 24.3% of these [7].
SA is reported in 0.02%–6.3% of appendicitis cases, representing up to 28.6% of chronic appendicitis in endemic areas [8]. The pathogenesis involves two mechanisms: a direct granulomatous reaction to egg deposition leading to tissue destruction, and an indirect mechanism where chronic inflammation and calcified ova cause fibrosis, obstruction, and secondary bacterial infection [9]. In our series, calcified ova were suspected radiologically in one case, consistent with the obstructive mechanism.
Clinically, SA is indistinguishable from ordinary acute appendicitis, as seen in our patients. Routine blood work may reveal leukocytosis; eosinophilia is inconsistent [10]. Imaging is rarely diagnostic, though mural calcifications may raise suspicion [11]. Histopathology remains the gold standard, revealing schistosomal ova with granulomatous or fibrotic changes [12].
Recent evidence suggests SA may be associated with higher risk of colorectal carcinoma due to chronic inflammation [13]. Therefore, recognition is important not only for surgical management but also for long-term surveillance. Definitive treatment includes appendectomy plus postoperative praziquantel, which is safe and effective in eradicating the infestation [12, 13].
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}