





Abstract
Bowel intussusception is a rare cause of obstruction in adults. Unlike the paediatric population, the etiology of adult intussusception is typically an underlying intestinal tumour, which can be benign or malignant, resulting in partial or complete mechanical ileus and corresponding symptoms. Diagnosing it through imaging techniques can be challenging and is sometimes only confirmed after an exploratory laparotomy. Surgical treatment in adults is often necessary because it aims not only to resolve the intussusception but also to address the underlying cause. We present three cases of surgically treated adult intussusception and discuss key points in managing this condition, based on a review of the literature.
Introduction
Intussusception is defined as the invagination of a section of the intestine into the lumen of its adjacent segment that may cause acute mechanical obstruction. In contrast to the pediatric population, in adult patients, it is an uncommon cause of acute abdomen. It is estimated that ~5% of all intussusceptions occur in adults, that ~5% of all intussusceptions arise in adults, and that ~5% of bowel obstructions in adults are the result of intussusception [1].
In adult intussusception, preoperative diagnosis cannot be established in approximately half of the cases [2]. The presentation of persistent ileus in a young adult with no prior abdominal surgery should prompt the surgeon to consider rare causes of obstruction, such as intussusception. According to the literature, computed tomography (CT) is the most helpful imaging modality. However, its accuracy remains moderate, ranging from 58% to 100% [3].
While the cause of intussusception in adult patients is often an underlying neoplasm, the location of the intussusception, symptoms, and neoplasm type (benign or malignant) vary significantly among patients, making surgical treatment challenging. In this study, we present three cases of adult intussusception with unique backgrounds, symptoms, and etiologies, and discuss key points for diagnosis and appropriate surgical treatment by reviewing the literature.
Case series
Three adult patients with bowel intussusception who underwent surgery in our department from 2012 to 2019 were included in the study.
The first case involved a 48-year-old woman who arrived at the emergency department with vomitting and diffuse abdominal pain over the past 24 hours. Her medical and surgical histories were unremarkable. Laboratory tests showed an elevated white blood cell (WBC) count of 17.4 mm3/μl (normal range 4.3–10.3 mm3/μl), while the C-reactive protein (CRP) level was normal at 0.4 mg/dl (normal range < 0.5 mg/dl). A plain abdominal X-ray in the upright position demonstrated air-fluid levels typical of intestinal obstruction (Fig. 1a), whereas the ultrasound examination was inconclusive. A CT scan revealed distention of the small intestine from the duodenum to the terminal ileum without identifying the cause of the obstruction. Initially, a nasogastric tube was placed for conservative management. After 48 hours, the patient’s condition and plain abdominal imaging (Fig. 1b) showed no signs of improvement, leading to the decision for an exploratory laparotomy.
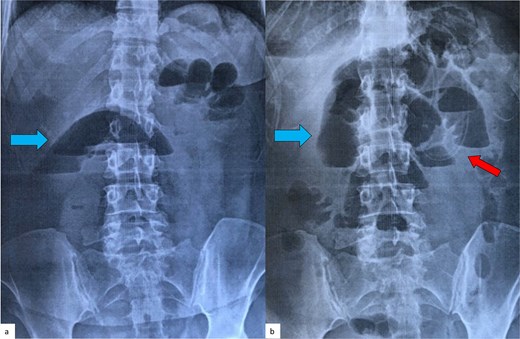
Plain abdominal radiograph of the patient (first case) in an upright position, on admission (a) and 48 hours later (b). Air-fluid levels (blue arrows), typical of small bowel obstruction, are clearly seen in both films, with no signs of improvement after conservative treatment with a nasogastric tube (red arrow).
This revealed an entero-enteric intussusception of the terminal ileum ~30 cm proximal to the ileocecal valve. An en bloc resection of the affected segment (~10 cm) and an end-to-end, hand-sewn anastomosis were performed. A small, intraluminal, palpable tumor was identified as the cause of the intussusception after close inspection of the specimen. The postoperative course was uneventful, and the patient was discharged on the 8th postoperative day. The histopathological and immunohistochemical report revealed a benign 2.5 cm submucosal neoplasm of mesenchymal origin with features of a neurofibroma (CD117, CD34, S100, and smooth muscle actin (SMA) negative).
The second case involved a 38-year-old woman with no prior medical history who presented to the emergency department with progressive, recurrent epigastric pain, vomiting, and diarrhea over the past ten days. Physical examination revealed tenderness and a palpable mass in the upper abdomen. All laboratory inflammation markers were within normal limits (WBC: 8.8 mm3/μl, CRP: 0.0 mg/dl). An ultrasound was initially performed, revealing a suspected bowel intussusception based on the characteristic “target sign” (Fig. 2).

Ultrasound examination of the patient (second case) on admission. The typical ‘target sign’ (arrow) is clearly demonstrated, raising the suspicion of a bowel intussusception.
This was later confirmed through a CT scan which depicted an abdominal “mass” with intestinal loops forming a multilayer concentric ring, extending from the ileocolic valve to the left upper abdomen, indicating an ileocolic intussusception (Fig. 3). Emergency surgery was performed, which further confirmed the CT findings by revealing an ileocolic intussusception of a long, ~40 cm segment of small bowel reaching the left colic flexure (Fig. 4). The decision was made to carefully realign the small intestine to minimize the extent of resection. After reduction, a palpable tumor was found in the caecum, identified as the cause of the intussusception. A small enterotomy of the ascending colon allowed direct visualization of the tumour, which appeared macroscopically suspicious for malignancy; therefore, a right colectomy with complete mesocolic excision and a hand-sewn side-to-side ileotransverse anastomosis was performed. Histological examination revealed a villous adenoma measuring 3.5 cm in diameter, located at the base of the appendix vermiformis, with mostly low-grade epithelial dysplasia and a few areas of high-grade dysplasia. The postoperative course was uneventful, and the patient was discharged on the sixth postoperative day.

Abdominal CT of the patient (second case) showing an abdominal ‘mass’ (arrow), consisting of intestinal loops forming a multilayer concentric ring, expanding from the ileocolic valve till the left upper abdomen and suggesting an ileocolic intussusception.
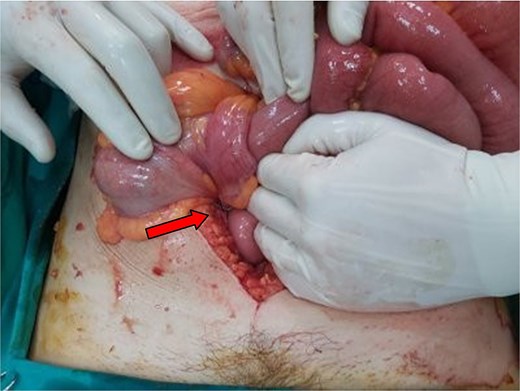
Intraoperative picture of the second case. The point of intusssception is annotated with an arrow.
The third case involved a 56-year-old woman who presented to our emergency department with acute epigastric pain lasting 24 hours and severe vomiting. She also reported losing 15 kilograms over the past year and having an episode of intestinal obstruction a year earlier, which was treated conservatively. Her medical history included familial adenomatous polyposis (FAP), hyperthyroidism, hypertrophic cardiomyopathy, atrial fibrillation, megaloblastic anemia, and hyperuricemia. Her surgical history comprised a subtotal colectomy with ileorectal anastomosis for FAP and endovascular repair of an abdominal aortic aneurysm. On examination, she had diffuse abdominal tenderness, slight distension, and a palpable mass in the left lower quadrant. Laboratory tests showed elevated inflammatory markers (WBC 12.9/mm3, CRP 7.1 mg/dl). Plain abdominal radiography revealed a single air-fluid level. CT scans demonstrated a large air-fluid level and suggested a possible jejunal intussusception, creating an abdominal mass measuring up to 7 cm and causing complete bowel lumen obstruction. An emergency laparotomy confirmed the diagnosis of jejuno-jejunal intussusception seen on CT. The affected segment was ~20 cm long and ischemic. A resection of ~65 cm of jejunum with a side-to-side anastomosis near the ligament of Treitz using a linear cutter was performed. Examination of the specimen revealed an intraluminal, polypoid mass as the cause of the intussusception. Histopathology identified a well-differentiated adenocarcinoma of the small intestine measuring 5.5 cm in diameter, with no lymph node metastasis. The postoperative course was uncomplicated, and the patient was discharged on the tenth postoperative day. The characteristics of the four patients are summarized in Table 1.
Characteristics of the four patients with intestinal intussusception
| Patient | Sex | Age | Imaging | Symptoms | Duration of symptoms | Surgical procedure | Type and cause of intussusception | Surgical technique | Histopathology |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 48 | PAR, US, CT | Diffuse abdominal pain, vomiting | 48 hours | Emergency | Ileoileal (small intestine neoplasm) | Enblock segmental ileal resection | Neurofibroma |
| 2 | F | 38 | US, CT | Reccurent epigastric pain, Vomiting 10 days | 10 days | Emergency | Ileocolic (caecum neoplasm) | Reduction, right hemicolectomy | Villous adenoma with partially high grade dysplasia |
| 3 | F | 56 | PAR, CT | Acute epigastric pain, vomiting | 24 hours | Emergency | Jejunojejunal (small intenstine neoplasm) | Enblock segmental jejunum resection | Adenocarcinoma |
PAR, plain abdominal radiograph; CT, computed tomography; US, ultrasound.
Discussion
Intussusception was first identified as a clinical entity in 1674 [4], and it is defined by the invagination of a proximal segment of the intestine into the adjacent distal segment. This occurs due to an abnormality in the peristaltic movement of the affected segment. The cause of this abnormality may be idiopathic or due to traction from an intra- or extraluminal lead point, such as a tumour. This can lead to intermittent or acute mechanical obstruction and, in the most severe cases, may impair mesenteric blood flow and cause ischemia in the affected segment [5].
Intestinal intussusception is most commonly found in the pediatric population (peak age 6 to 18 months), but rarely—~1%–5% of cases—can also cause bowel obstruction in adults [6]. Literature indicates that the average age of adult patients with intussusception is 50 years, with no gender predominance [5]. However, all three cases we present were female, with an average age of 44. Similar to our findings, Wang et al. [7] observed a male-to-female ratio of 1/1.3 and a female average age of 47 in a large retrospective series of 41 cases.
Regarding the location of intussusception in adult patients, the small bowel is affected more frequently than the colon, with the most common types being ileocolic, enteroenteric, and colocolic [8]. Conversely, the upper gastrointestinal tract is rarely involved, with only a few cases of gastroduodenal intussusception described in the literature [9]. Even rarer are colorectal [10] and coloanal intussusception [11]. In our series, we report two cases of enteroenteric and one of ileocolic intussusception.
Unlike children, where the etiology of intestinal intussusception is mainly idiopathic, in adult patients, an underlying cause is responsible for ~90% of cases [1, 6, 12, 13]. In the small bowel, benign (hamartoma, hemangioma, inflammatory polyp, neurofibroma) or malignant (GIST, lymphoma, leiomyosarcoma, neuroendocrine tumor, metastatic melanoma) neoplasms account for two-thirds of the non-idiopathic cases, while Meckel's diverticulum, adhesions, or submucosal haemorrhage are less common causes. In the colon, neoplasms such as adenomas, lipomas, and adenocarcinomas can cause intussusception [5]. In all our cases, the underlying cause was a neoplasm.
Regarding the clinical presentation of the disease, the classic triad of symptoms commonly seen in children—acute abdominal pain with sudden onset, palpable mass, and bloody stool [14]—is rarely observed in adult patients [15]. Symptoms of adult intussusception vary widely and can be acute, chronic, or intermittent. The predominant symptoms include abdominal pain accompanied by signs of complete or partial bowel obstruction, such as nausea, vomiting, abdominal distention, and constipation, with duration ranging from days to weeks or even months [6, 12]. Additionally, rectal bleeding, diarrhea, or the presence of an abdominal mass may indicate intussusception [5, 7]. A palpable mass is mainly found in colonic lesions in 10%–30% of patients [5, 7], but in our series, it was detected in two patients with small bowel intussusception. A notable feature of these cases was that the proximal part of the intestine (intususceptum) was very long—40 cm in the second case and 65 cm in the third. The primary symptom observed in all our patients was abdominal pain of variable duration, ranging from 24 hours to 10 days.
The differential diagnosis of adult intussusception includes all conditions related to obstructive ileus or an acute abdomen. Because it lacks specific symptoms and is rare, diagnosis can be difficult, often leading to delayed surgical treatment and complications such as bowel ischemia, widespread peritonitis, and shock. Additionally, the sensitivity and specificity of imaging techniques are moderate in adult intussusception, and the choice of imaging varies among patients depending on the suspected diagnosis.
A plain abdominal radiograph taken in an upright position can reveal signs of intestinal obstruction, such as distended bowel loops or absence of air in the large bowel, or perforation, indicated by free air under the diaphragm. It is a cost-effective and sensitive method for diagnosing bowel obstruction, but it lacks specificity in pinpointing the exact location and cause, such as intussusception [16]. Conversely, contrast studies like barium enema may aid in diagnosing colonic intussusception, but their use is limited in adult patients, especially in emergency situations [15].
Ultrasound is a noninvasive, radiation-free technique; therefore, it is considered the preferred imaging modality for diagnosing intussusception in children and may also be diagnostic in adult patients. The characteristic ‘target or bull's eye sign’ seen from the intussuscepted loops forming an external ring around the intussusceptum can be depicted by an experienced radiologist [17] (Fig. 2). In paediatric patients, the reported sensitivity of this method is nearly 100%. However, in adult patients, it is significantly lower (30%–60%) [6, 7, 18]. According to Wang et al., if a palpable mass is present, the method's diagnostic accuracy improves considerably, reaching 91% [7]. Of the three cases we present, ultrasound was performed in two patients with epigastric pain to rule out gallbladder issues. It was diagnostic only in the second case, which also had a palpable mass. Regarding CT scan, it seems to be the most useful diagnostic tool in adult intussusception, with reported accuracy ranging from 78% to 100% [6, 7, 12, 18, 19]. Intussusception appears as an inhomogeneous mass with a central fatty area and enhanced blood vessels (representing the intussuscepted mesentery), along with multiple, eccentric layers indicating thickened segments of bowel (the intussusceptum and intussuscipiens) [20]. Additionally, CT can offer indirect clues in malignancy cases (such as metastatic liver lesions or lymphadenopathy). However, in most cases, it cannot identify the primary tumor causing the intussusception.
Finally, in addition to a CT scan, preoperative colonoscopy is a valuable tool for distinguishing benign from malignant lesions and can even be therapeutic by realigning the intussusception. It should be noted, however, that availability in emergency settings varies greatly among hospitals [13].
Regarding treatment of the disease, in contrast to pediatric intussusception, which is most often ileocolic and idiopathic, conservative approaches such as pneumatic or contrast enemas are not recommended in adult intussusception. Surgical intervention remains the gold standard for definitively treating the underlying cause. However, some aspects of the treatment, including operative technique and the extent of resection, are still debated. For example, several authors support reducing the intussusception before resecting the pathological segment [18, 21]. Conversely, others favor primary en bloc resection without reduction to reduce unnecessary manipulation of the specimen and decrease the risk of bacterial and tumor spillage in cases of malignancy [8, 15]. Because preoperative evaluation of the underlying cause is often unavailable, the decision should be tailored to intraoperative findings—such as patient age, bowel condition, intussusception location, length of the intussusceptum, and suspicion of malignancy. When the bowel appears inflamed, ischemic, or friable, it is advisable not to attempt reduction but to proceed directly with resection. Due to the high risk of malignancy, colonic lesions should not be reduced, and oncologic hemicolectomy with adequate lymphadenectomy should be performed. Limited resection after reduction of an intussusception is justified only if a benign diagnosis has been established pre- or intraoperatively, or if resection would cause short gut syndrome. In cases of a very long intussusceptum without signs of ischemia (like the second case), careful reduction prior to resection should be considered to avoid unnecessary removal of the entire bowel segment. Finally, intraoperative colonoscopy and diagnostic enterotomy may serve as additional tools to better evaluate the underlying cause of the intussusception and reduce the extent of resection [13].
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This case series received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. As it was a non-interventional, retrospective/observational study, no experimental intervention or modification of patient management was required. According to national and European regulations, our institution’s ethics committee waived the need for formal approval for this publication. All data and figures were anonymized prior to analysis to ensure confidentiality and privacy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}