





Abstract
Giant Meckel’s diverticula (GMD), characterized by a diameter over 5 cm, are a rare manifestation of the most common congenital gastrointestinal anomaly. GMDs challenge the conventional understanding of Meckel’s diverticulum. Their detection may be linked to complications such as inflammation, perforation, or obstruction, which are more frequent in larger lesions. This report presents an unusual case of GMD found incidentally during surgery for acute appendicitis, representing the first documented instance in the English-speaking Caribbean. It emphasizes the diagnostic difficulties associated with these lesions, the possibility of additional pathology, and the reason for surgical removal, even when they are discovered incidentally.
Introduction
Meckel’s diverticulum (MD), first identified by Hildanus and subsequently by Johan Friederich Meckel in the early 19th century, is the most common congenital anomaly of the gastrointestinal tract, with an estimated occurrence of 0.2% to 4% [1, 2]. These diverticula are usually found up to 200 cm proximal to the ileocecal valve and measure between 0.4 and 11.0 cm in length and 0.3 to 7.0 cm in diameter [3]. Giant Meckel’s Diverticula (GMD), those over 5 cm in diameter, are even more rare, with limited descriptions in existing literature and, to the author’s knowledge, have never been described in the English-speaking Caribbean. Here, the authors present a case of an incidental Giant MD, along with its management.
Case report
A thirty-year-old man with no chronic illnesses presented to the emergency department with a three-day history of generalized abdominal pain and vomiting. His surgical history was notable for a previous admission one year prior for Computed Tomographic (CT) scan confirmed uncomplicated acute appendicitis that was managed non-operatively. His current complaints included gradually worsening right lower quadrant pain that later became generalized. The history was also positive for multiple episodes of vomiting that contained previously ingested food and later bile-stained fluid. The patient also complained of loose, watery stool and progressive global abdominal distension. On the day before presentation, he experienced subjective fever with chills and rigors. Physical examination revealed abdominal distension with marked tenderness in the lower abdomen, guarding, and rebound tenderness, most pronounced in the right iliac fossa. No palpable masses or organomegaly were noted; bowel sounds were present but reduced. Cardiovascular, respiratory, and neurological examinations were normal. A CT scan of the abdomen and pelvis showed the following (Figs 1 and 2):
A dilated appendix measuring 1.6 cm in diameter with peri-appendiceal inflammatory changes. A 1.1 cm fluid focus with peripheral enhancement was seen, consistent with focal perforation.
A 10.9 cm (AP) × 7.2 cm (W) focus that appeared to arise from a loop of ileum, concerning for a giant small bowel diverticulum
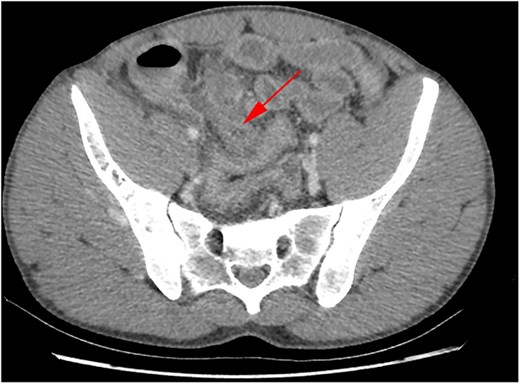
CT abdomen/pelvis axial view demonstrating inflamed appendix.

CT abdomen/pelvis axial view demonstrating small bowel diverticulum.
After intravascular fluid resuscitation, exploratory laparotomy was performed with findings below (Fig. 3):
300 cc seropurulent pelvic collection within the right lower quadrant
A grossly dilated, inflamed appendix with 0.5 cm perforation midway along its length
20 × 12 cm diverticulum to ileum, approximately 60 cm from the ileocecal valve
Fecalith in situ
Enlarged mesenteric lymph nodes
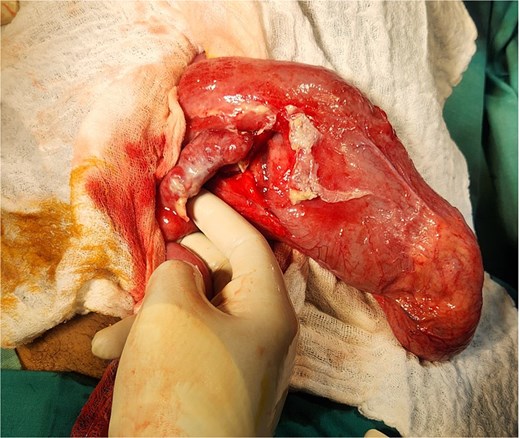
Intraoperative picture demonstrating MD and inflamed appendix.
An intraoperative diagnosis of acute ruptured appendicitis with and giant MD was made. An appendectomy was performed, followed by a segmental ileal resection incorporating the diverticulum (Fig. 4). A primary, end-to-end, hand-sewn, single-layer ileo-ileal anastomosis was constructed using 2–0 silk.
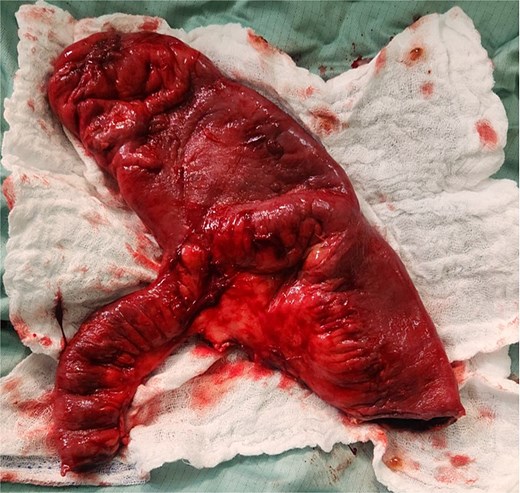
Resected specimen showing Giant MD.
The postoperative course was unremarkable, and the patient was discharged on day three. Gross pathological examination revealed a T-shaped segment of the small bowel, including a segment continuous with a 23 × 13 cm dilated portion. Histological appraisal revealed an evagination of the wall involving all layers, accompanied by significant oedema and congestion of the submucosa. No heterotopic mucosa was identified. Acute inflammation and fibrin deposition were observed in the serosa. These findings were consistent with Giant MD with diverticulitis. The vermiform appendix specimen exhibited acute inflammatory changes with neutrophilic infiltration across all layers, indicative of acute appendicitis.
Discussion
MD is a congenital anomaly resulting from incomplete closure of the omphalomesenteric (Vitelline) duct during week’s five to seven of fetal development [1]. GMD contradict the commonly quoted ‘laws of 2s’ that define their typical presentation, and as such, they bear special consideration. Though only being symptomatic in 5% of patients, larger diverticula are associated with increased incidence of obstructive and inflammatory presentations [4, 5]. GMDs are also associated with increased rates of heterotopic mucosae, which may impact the complication rate [6]. MD have also been associated with increased malignancy potential, though this risk is less than 5%; this may be increased in GMDs [7]. Debate continues regarding the management of asymptomatic diverticula discovered incidentally on imaging or during surgery. Certain authors suggest that diverticulectomy or segmental resection be employed due to the risk of symptomatology, delays in treatment due to diagnostic uncertainty and the minimal morbidity associated with resection [8]. While others favor a conservative approach due to the low lifetime complication risk and attendant risks associated with surgery, we favor a resection-based approach, particularly in GMDs, as was employed in the index patient. The presence of the large fecalith within the diverticulum further reinforced the decision to proceed, given the potential for intestinal obstruction. We therefore propose that the presence of a fecalith be an indication for resection. To the best of our knowledge, this represents the first publication in English-based literature documenting the coexistence of Giant Meckel’s diverticulitis and acute appendicitis.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}