





Abstract
Lipoma is a benign mesenchymal tumor composed of adipose tissue encapsulated by connective tissue. Omental lipoma can cause large intra-abdominal mass which itself a rare finding (Li JXJ, Giddings HL, Owen G. Omental lipoma: a rare cause of a giant intra-abdominal mass. J Surg Case Rep 2022;2022:rjac160. 10.1093/jscr/rjac160). It can be present as mass in area around ovaries and fallopian tube mimicking adnexal mass. We hereby describe a case of a 40-year female who presents as non-specific abdominal pain, sensation of heaviness in pelvic region, and increase frequency of micturition, with further imaging, modality omental lipoma was encountered, exploratory laparotomy mass arising from broad ligament and complete excision was performed. Further confirmed by histopathology examination.
Introduction
Omental lipoma is an uncommon abdominal benign tumor of mature fat cells, which is usually asymptomatic [1]. If the tumor encase around ovaries/fallopian tube, it can mimic as adnexal mass causing diagnostic delima. It unusual origin from broad ligament as having limited amount of fat, which makes it a rare entity. Lipoma of broad ligament is of interest because of gynecological diagnostic problem, different surgical extirpation [2]. We present a case of broad ligament omental lipoma mimicking adnexal mass, highly diagnostic and therapeutic challenge.
Case
A 40-year female presented to outpatient department with 1 year history of non-specific abdominal pain. She had history of sensation of heaviness at pelvis region and increase frequency of micturition with no other urinary symptoms. She had no significant medical, surgical, and gynecological history with unremarkable family history. On physical examination, she looks healthy, consciousness. Her vitals were in normal range. Per abdominal examination: soft to palpate with mass felt ~12 × 12 cm at right lower quadrant, non-tender, and bowel sounds present. Laboratory investigation revealed complete blood count, renal function test, liver function test, prothrombin time/international normalize ratio were in normal range, cancer antigen (CA)-19.9: 32.7 μ/ml, carcinoembryonic antigen: 5.37 ng/ml, CA--125: 8.9 μ/ml. Ultrasonography of abdomen and pelvis revealed well-defined hypoechoic cystic lesion measuring 12.3 cm × 9.4 cm size with septa in right adnexa and right adnexal mass. Contrast-enhanced computed tomography (CECT) abdomen showed well-defined hypodense abdominopelvis lesion of fat density in right side measure 13.2 × 8.5 × 11.8 cm contain thin internal septa with craniocaudal extension from L4 to S5 vertebrae, abutting fundus of uterus, right ureterprximal, rt external and internal iliac vessel with no lymphadenopathy, and ascites (Fig. 1).
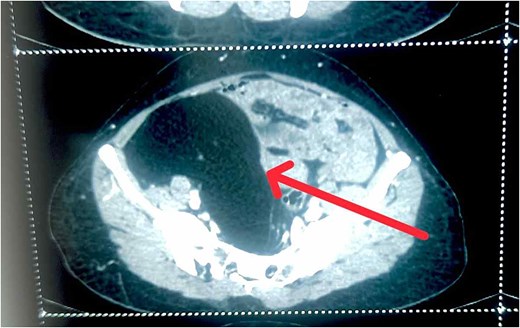
CECT abdomen showing well-defined hypodense abdominopelvis lesion of fat density in right side.
After counseling and discussion of malignant potential with the patient, decision to treat this mass by open surgical procedure was reached [3]. Double J stenting was place in right ureter prior to procedure to reveal the compression on right ureter. An exploratory laparotomy through midline incision having safe entry in abdominal cavity achieved, intraoperative finding showed well-encapsulated mass ~15 × 12 cm in right iliac fossa (Fig. 2) arising from broad ligament encasing rt fallopian tube, rt ovary, and feeder vessel from rt uteric artery. Excision was safely performed separating from surrounding; firm fatty mass was 15 × 12 cm weighs ~2077 kg (Fig. 3). Surgery was followed by uneventful recovery period with maintaining good health without any complications. Patient was discharged on stable condition. Histopathology revealed well-defined capsulated and lobulated lesion of mature fat uniform in size with intervene fibrous septa with small arborizing vessel most likely lipoma (Fig. 4).

Intraoperative finding showed well-encapsulated mass ~15 × 12 cm in right iliac fossa.

Gross surgical specimen showing, firm fatty mass was 15 × 12 cm weighs ~2077 kg.
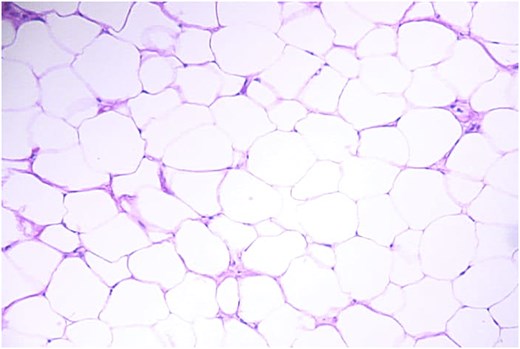
Histopathology revealed well-defined capsulated and lobulated lesion of mature fat uniform in size with intervene fibrous septa with small arborizing vessel most likely lipoma.
Discussion
Although lipoma is most common mesenchymal tumor, intra-abdominal lipoma is rarely seeing with omental lipoma arising from broad ligament exceed scarcely. The presence of non-specific abdominal pain, sensation of heaviness in pelvic region with increased frequency of micturition may be due to it’s size or pressure on adjacent region, arises a diagnostic dilemma of vague differential diagnosis. Radiological modality as ultrasonography and computed tomography (CT) scan of abdomen are preferred imaging study for abdominal lipoma. Further, magnetic resonance imaging (MRI) abdomen provides excellent tissue characterization and should be confirmed by his pathological examination [4]. Treatment of such case only includes complete surgical excision but also efforts to avoid or it’s recurrence [5, 6].
Conclusion
This case highlights a rare presentation of omental lipoma arising from broad ligament with unusual symptoms. Though it’s unusually diagnosed, one should consider differential diagnosis of intra-abdominal mass. Accurate diagnostic imaging with CT scan and MRI of abdomen with confirmation by histopathology should be reserved. Definitive management is complete surgical excision in most case with lower recurrence rate [7].
Conflict of interest statement
None declared.
Funding
None declared.
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}