





Abstract
Feeding jejunostomy is performed commonly following esophagectomy to ensure postoperative nutritional support. However, it can occasionally lead to rare complications, such as intussusception. Adult intussusception, especially secondary to a feeding jejunostomy, is an uncommon occurrence. Timely diagnosis and surgical intervention are essential to treat this potentially life-threatening condition. We report a 69-year-old male, who has received neoadjuvant chemoradiotherapy followed by a thoraco-laparoscopic Ivor Lewis esophagectomy and a feeding jejunostomy. The immediate postoperative course was uneventful. However he presented with acute abdominal symptoms at 6 weeks. A contrast-enhanced computed tomography scan of the abdomen revealed intussusception at the site of the feeding jejunostomy. The patient underwent emergency exploratory laparotomy, where the diagnosis was confirmed, and resection and anastomosis of the involved bowel segment was performed. This case highlights a rare complication of jejunostomy-induced intussusception. A high index of suspicion and prompt surgical management are crucial to prevent adverse outcomes in such cases.
Introduction
Feeding jejunostomy is performed commonly to maintain nutritional support in patients, who are undergoing major upper gastrointestinal surgery, particularly esophageal cancer [1]. While complications such as tube dislodgement and infection are more common, intussusception, especially in adults, is a rare occurrence [2]. Adult intussusception accounts for only 1%–5% of all cases and is typically associated with a pathological lead point such as a tumor or adhesions [3]. This case report presents a rare instance of jejunostomy-induced intussusception, discussing its clinical management and importance in surgical practice.
Case presentation
A 69-year-old gentleman who was diagnosed with carcinoma of the lower esophagus. He underwent neoadjuvant chemoradiotherapy as per the CROSS protocol followed by a thoraco-laparoscopic Ivor Lewis esophagectomy and a feeding jejunostomy. The postoperative period was uneventful, and the patient was discharged in stable condition.
Six weeks later, the patient presented with acute abdominal pain and vomiting. A physical examination revealed mild abdominal distension with tenderness upon palpation. Given the patient’s medical history, the clinical presentation raised concerns of a possible mechanical obstruction. A contrast-enhanced computed tomography (CT) scan of the abdomen revealed intussusception at the site of the feeding jejunostomy, with a bowel segment telescoping into itself, leading to obstruction (Fig. 1).
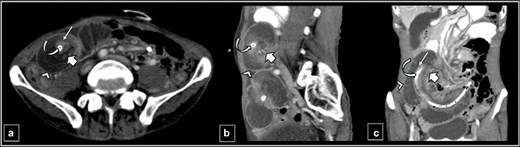
Contrast-enhanced CT abdomen images of axial (a), sagittal (b), and coronal (c) sections showing the jejunojejunal intussusception with a target sign. The structures from outer to inner: grossly dilated intussuscipiens-distal jejunal loop (arrow head), the intussusceptum-proximal jejunal loop (long thin arrow), proximal jejunal mesenteric fat and the vessels (short thick arrow) within the intussuscipiens, and the feeding jejunostomy tube (curved arrow) within the intussusceptum.
The patient was taken for an emergency exploratory laparotomy. Intraoperatively, intussusception was confirmed at the site of the feeding jejunostomy (Fig. 2). A segmental resection of the affected bowel, including the jejunostomy site, was performed, and continuity was restored via an end-to-end anastomosis. The patient had an uneventful postoperative recovery and was discharged in stable condition. At the 6-month follow-up, the patient remained asymptomatic and disease-free.
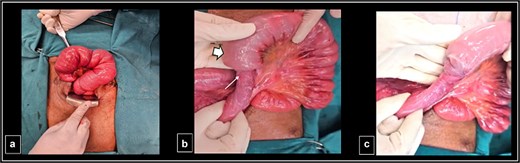
Intraoperative findings. (a) Significant small bowel dilatation. (b) Intussusception part identified with intussusceptum-proximal jejunal loop (long thin arrow) and dilated intussuscipiens-distal jejunal loop (short thick arrow). (c) Post reduction of intussusception.
Discussion
Adult intussusception is rare and typically arises secondary to a pathological condition, such as a tumor, adhesions, or postoperative changes [1]. Intussusception related to feeding jejunostomy is a much rarer complication, with limited cases reported in the literature [4]. The jejunostomy tube likely acted as the lead point for the intussusception in this case, with mechanical irritation and abnormal peristalsis contributing to the complication [5].
Feeding jejunostomy is commonly performed in patients undergoing major gastrointestinal surgeries, such as esophagectomy, where postoperative nutritional support is critical. Although more common complications include infection, leakage, and tube dislodgment, intussusception is a rare but serious complication [4]. It is important for clinicians to maintain a high index of suspicion, especially in patients presenting with signs of acute abdominal pain and bowel obstruction postoperatively. The clinical presentation of intussusception in adults is often nonspecific, typically mimicking other causes of bowel obstruction [6]. Imaging, particularly CT scans, plays a crucial role in diagnosing intussusception, with a sensitivity rate of nearly 100% [7]. In this case, the CT scan revealed classic signs of intussusception, allowing for timely surgical intervention. Surgical intervention remains the definitive treatment for adult intussusception, particularly when it is associated with a feeding jejunostomy. Resection of the affected bowel segment and restoration of continuity is the preferred treatment [8].
Polyvinyl chloride feeding tubes, commonly used in procedures like feeding jejunostomy, can stiffen over time due to prolonged exposure to body heat, digestive fluids, and environmental factors. This increased rigidity may contribute to complications such as intussusception, as the hardened tube can disrupt normal peristalsis and cause mechanical irritation, potentially serving as a lead point for the condition [9]. To mitigate these risks, it is advisable to use more flexible and biocompatible materials, such as silicone or polyurethane, for long-term tube placement [9]. These materials are less prone to hardening and can reduce the likelihood of complications. Regular replacement of feeding tubes before significant hardening occurs and close clinical monitoring for early signs of intussusception are also essential preventive measures. Implementing these strategies can help reduce the incidence of complications associated with feeding jejunostomy.
Conclusion
This case highlights the rare complication of jejunostomy-induced intussusception. A high index of suspicion and prompt surgical management are crucial to prevent adverse outcomes in such cases.
Conflict of interest statement
None declared.
Funding
None declared.
Data availability
Data can be provided on request.

{kind=link}
{kind=link}