





Abstract
We reported a case of a 45-year-old male patient with trans-scaphoid trans-triquetrum lunate dorsal dislocation combined with fracture of ulnar and radius with forearm compartment syndrome. During the initial surgery, the scaphoid fracture end was mistakenly fixed together with the triquetrum fracture end, leading to an erroneous reduction, which was later identified and corrected through a secondary reduction. It is emphasized that in patients with lunate dislocation and concomitant scaphoid and triquetrum fractures, accurate identification of the fracture ends of both the scaphoid and triquetrum bones is critical to avoid erroneous fixation. Furthermore, the presence of ulnar and radial fractures increases the risk of forearm compartment syndrome.
Introduction
Trans-scaphoid lunate dislocation is a relatively uncommon injury [1, 2], and the simultaneous occurrence of trans-scaphoid, trans-triquetrum lunate dorsal dislocation, along with fractures of the ulna and radius and forearm compartment syndrome is even rarer. In this case, difficulties were encountered in correctly identifying the scaphoid and triquetrum fracture ends during the initial surgery, leading to the erroneous fixation of the scaphoid fracture end together with the triquetrum fracture end. It is crucial for clinicians to accurately identify the fracture ends when managing multiple wrist fractures and dislocations involving the carpal bones. The patients and their families were informed that the case data would be submitted for publication and consented.
Case presentation
A 45-year-old manual worker presented following a fall from a scaffold about 2 m high. On examination, significant swelling of the left forearm and wrist was noted, with the disappearance of arterial pulsation and pallor of the hand. The patient also reported progressive paresthesia in the left hand, and motor weakness was observed. Emergency X-ray and wrist computed tomography (CT) scans revealed fractures of the ulna and radius, a dorsal fracture of the distal radius with dislocation of the inferior radioulnar joint, and dorsal dislocation of the lunate bone. Additionally, a scaphoid fracture, partially displaced toward the volar side was noted, along with a concomitant triquetrum fracture (Fig. 1). An emergency wound debridement and decompression procedure was performed. During the surgical intervention, a lazy S-shaped incision, ~25.0 cm in length, was made on the left palm and the palmar side of the forearm. Fasciotomy was conducted to release the deep fascia (Fig. 2). Intraoperatively, the wrist joint capsule was found to be damaged, exposing a scaphoid fracture that had fragmented into two pieces, with one fragment displaced toward the volar side. Additionally, the triquetrum bone was fractured into two pieces, with one fragment displaced toward the radius (Fig. 2). Following fracture reduction, the volar fragment of the scaphoid fracture was fixed in conjunction with the triquetrum fracture fragment using two Kirschner wires. The radial-carpal joint was also stabilized with two K-wires. Postoperative X-ray images revealed a poor reduction of the fracture ends, while the position of the lunate bone was generally considered acceptable (Fig. 3).
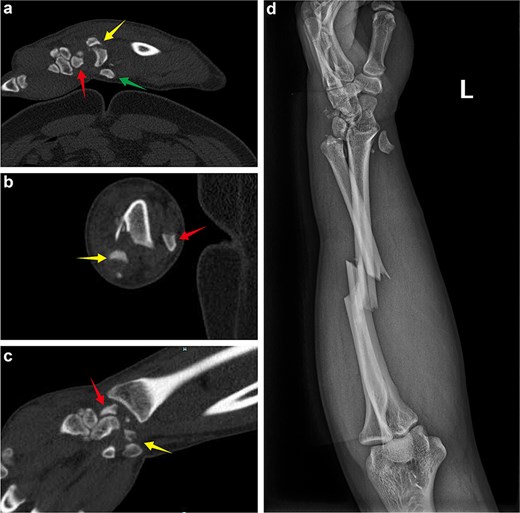
(a) Emergency admission sagittal CT of the wrist showing the dorsal dislocation of the lunate, the fracture end of scaphoid bone in the wrist joint, and the volar displacement of the scaphoid bone. (b) Axial CT of the wrist showing the dorsal displacement of the lunate and the fracture end of the scaphoid bone. (c) Coronal CT of the wrist showing the fracture end of the scaphoid bone and the fracture end of the triquetrum bone. (d) Emergency admission X-ray revealing the dorsal dislocation of the lunate bone, volar displacement of the scaphoid fracture end, injury to the inferior radioulnar joint, and a middle radius-ulnar fracture.
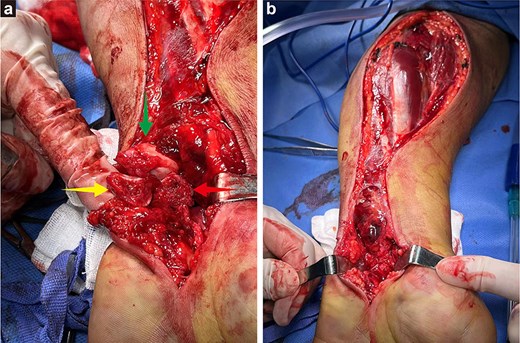
(a) In the first operation, arrows indicate the fracture end of the triquetrum bone, the dislocated lunate (reduced from the dorsal side), and the volar displacement of the scaphoid bone. (b) A lazy S-shaped fasciotomy was performed along the volar aspect of the forearm, indicating total decompression of the volar compartment and wrist during the first surgery.

(a and b) After the first operation, X-ray images revealed that the volar displaced scaphoid fracture end had been incorrectly fixed to triquetrum fracture end. Temporary fixation of the unstable wrist joint was achieved using Kirschner wires, while the ulna and radius were not fixed. The lunate bone had not yet been completely repositioned.
The forearm wound was closed after 1 week. After 2 weeks, the patient underwent surgery for carpal bone and ulnar radius fractures through a dorsal incision. The disarranged lunate, scaphoid, and triquetrum bones were realigned. Due to the incorrect fixation of the scaphoid and triquetrum fracture ends, the original Kirschner wires were removed, and a buried screw was used to refix the fracture end of the scaphoid bone. Kirschner wires and a locking plate were then used to restore the carpal alignment (Fig. 4). At the radial sigmoid notch site, small bone fragment was identified and fixed with a K-wire. Postoperative fluoroscopy revealed that the fracture ends were in good position, and the internal fixation was properly aligned (Fig. 5). After 6 months, the steel plate and Kirschner wires were removed from the wrist, and the patient gradually began functional exercises (Fig. 6).
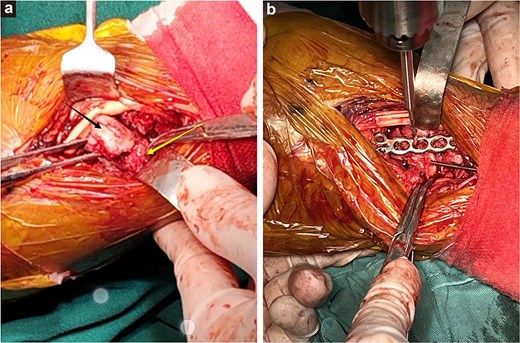
(a) The free scaphoid bone (black arrow) was mistakenly repositioned with the triquetrum bone (yellow arrow). (b) The wrist bones were stabilized with a small plate during surgery, maintaining the stability of the radiocarpal joint.
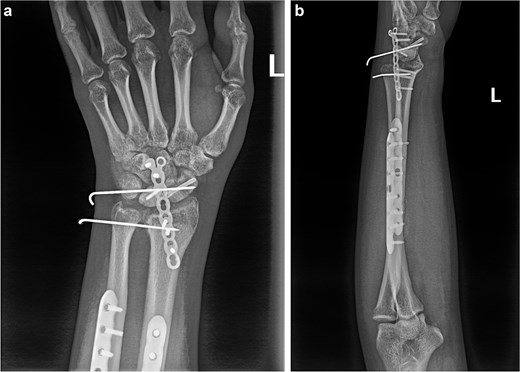
(a and b) Anterior and lateral views of the wrist joint following the second postoperative intervention, demonstrated satisfactory reduction of the fracture ends of the wrist bones, and the lunate bone had been relocated.

(a and b) Anterior and lateral views of the wrist joint after 6-month follow-up.
Discussion
In this instance, the mechanism of injury in this patient may have been extreme dorsal extension of the wrist joint during a high fall. The scaphoid and triquetrum bones fractured upon impact with the distal articular surface of the radius and ulna, with the proximal scaphoid fracture end displaced toward the volar side. Subsequently, the lunate was compressed between the distal radius and capitate, leading to its dislocation toward the dorsal side. Continued force resulted in transverse fractures of both the ulna and radius. This case is reported to highlight the following.
Upon admission, an open reduction and temporary Kirschner wire fixation were performed. Due to the inexperience of the emergency physician, the volarly displaced scaphoid fracture end was incorrectly fixed to the triquetrum fracture end. The reasons for this error are analyzed as follows: the dislocation of the lunate, along with scaphoid and triquetrum fractures, brought the fracture ends closer together, making mistaken reduction more likely. Additionally, the dorsal fracture of the distal radius at the inferior radioulnar joint complicated the reduction of the wrist bone fractures. The key to the treatment of wrist bone fractures and dislocations is the restoration of the position between the lunate and capitate bones, followed by early reduction and fixation of the scaphoid to prevent ischemic necrosis. It has been reported that in cases of scaphoid fracture with lunate dislocation, the lunate bone should be reduced first, after which the scaphoid fracture is stabilized with a buried screw, the lunate, and capitate are fixed by Kirschner wire, and the wrist ligament structure is repaired. This approach has demonstrated favorable outcomes [1]. The diagnosis of compartment syndrome is primarily based on two main factors: a high index of suspicion and an understanding of the variable clinical presentation [3]. In this case, the disappearance of the arterial pulse and the paleness of the hand, coupled with the patient's reports of progressive paresthesia and the observed motor dysfunction, warranted early incision, and decompression, which was determined to be highly appropriate. The question of whether distal ulnar radius fractures with forearm compartment syndrome should be initially fixed remains a subject of debate. Concerns have been raised regarding the potential for early internal fixation to increase the risk of infection. However, some studies have suggested that the use of locking compression plates for external fixation has shown favorable outcomes in the treatment of open fractures of the ulna and radius [4]. This approach has been found to restore limb length, provide stability, facilitate soft tissue healing, and prevent displaced bone blocks from damaging vascular and neural structures.
Conclusion
The authors concluded that in cases of multiple carpal fractures with lunate dislocation, inexperienced clinicians may encounter difficulties in distinguishing the fracture at the narrowest incision. Adequate exposure of the fracture ends may be required, along with a thorough understanding of the anatomy of the various carpal bones. Additionally, the combination of ulnar and radial fractures may easily complicate the condition with forearm compartment syndrome.
Author contributions
Z.L. collected the information and wrote the report. G.H.J. assisted with the writing of the report and collected X-rays. W.G.X. assisted with the surgical operation. Z.L. had the initial idea for the report and is guarantor. All authors read and approved the final manuscript.
Conflict of interest statement
None declared.
Funding
None declared.
Data availability
Please contact author for data requests.
References
Alshehri D, Mousa A, Al Ahmadi B.
Hanandeh A, Mani VR, Bauer P, et al.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}