





Abstract
Situs inversus is a rare congenital anomaly that results in the transposition of the abdominal organs, leading to atypical clinical presentations, such as left-sided appendicitis. Acute appendicitis is the most common cause of right iliac fossa pain; however, its occurrence on the left side is exceedingly rare and often leads to diagnostic delays, which may result in serious complications such as peritonitis if not promptly addressed. Imaging modalities, particularly computed tomography (CT), play a critical role in the anatomical and pathological diagnosis, thereby guiding appropriate surgical management. We present the case of a 67-year-old patient with a history of ileocecal tuberculosis, myocardial infarction, and ischemic stroke, who was admitted with left iliac fossa pain, initially suspected to be due to sigmoiditis. A CT scan revealed situs inversus with high-positioned left-sided appendicitis, prompting the indication for urgent laparoscopy. Surgical exploration confirmed a retrocecal appendicitis with minimal peritoneal effusion, and an appendectomy was performed.
Introduction
Situs inversus totalis (SIT) is a rare congenital anomaly characterized by a complete inversion of thoracic and abdominal organs, with an incidence ranging from 1 in 10 000 to 1 in 50 000 individuals [1, 2]. This condition alters the normal anatomy of the human body, which can lead to diagnostic challenges, particularly when it presents with common conditions in atypical locations [3]. Acute appendicitis, the most frequent cause of pain in the right iliac fossa, is extremely rare when it occurs on the left side due to organ rotation. This phenomenon can result in diagnostic delays and serious complications if not managed promptly. Imaging techniques, particularly computed tomography (CT), are essential for an accurate diagnosis both anatomically and pathologically, guiding the appropriate surgical approach.
Observation
We report the case of a 67-year-old patient with significant medical history, including ileocecal tuberculosis diagnosed at age 40 Not documented, followed by a myocardial infarction (MI) at age 60, for which coronary bypass surgery was performed. The patient also had a history of an ischemic stroke, treated medically.
The patient was admitted to the emergency department with localized pain in the left iliac fossa and flank, clinically suggesting sigmoiditis, particularly considering his age and dietary habits. On clinical examination, the patient was conscious and hemodynamically stable (blood pressure: 15/7, heart rate: 76 bpm), with a respiratory rate of 18 cycles/min. Abdominal examination revealed generalized guarding of the left flank extending to the left iliac fossa. Digital rectal examination showed no particular findings. The examination of other systems was normal. Biological tests revealed leukocytosis at 23 000/mm3 with a CRP of 1 mg/L. A urinary culture was negative.
An urgent CT scan revealed situs inversus (Fig. 1) with left-sided high-positioned appendicitis (Fig. 2).
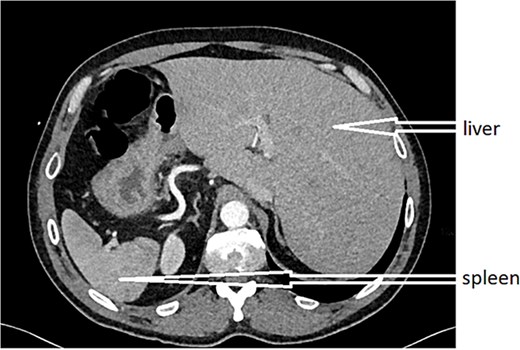
CT scan revealed situs inversus.
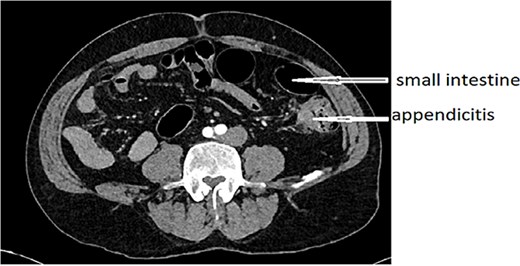
Left-sided high-positioned appendicitis.
After obtaining informed consent and providing the patient with information about the case, he was transferred to the operating room after preparation, including rehydration, proton pump inhibitor (PPI), antibiotic therapy, and analgesia. Urgent exploratory laparoscopy confirmed the CT findings: retrocecal appendicitis with minimal peritoneal effusion (Fig. 3) in the Douglas pouch. A careful dissection of the appendix from its mesentery was performed, followed by appendectomy (Fig. 4), lavage, and drainage.
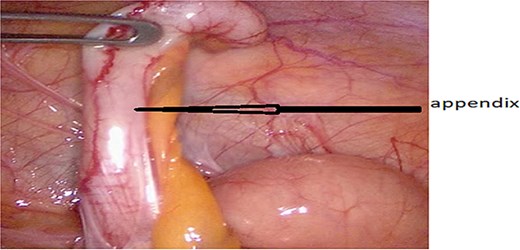
Retrocecal appendicitis with minimal peritoneal effusion.
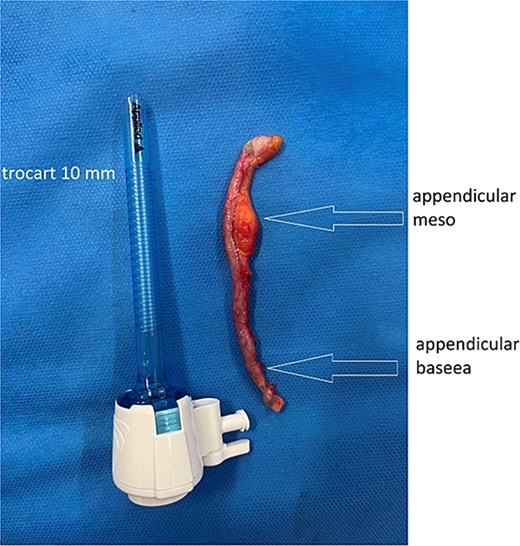
Appendectomy.
Discussion
Congenital anomalies of the gastrointestinal tract represent a major cause of morbidity, particularly in children [4], but they can also be observed, albeit more rarely, in adults [5], as in our case.
The clinical case presented in this study highlights an unusual discovery of this anomaly in the form of appendicitis with left-lateralized clinical signs [6, 7]. Although acute appendicitis accounts for approximately one-third of abdominal emergencies, its left-sided occurrence remains exceptional [8]. This can lead to diagnostic errors, particularly in distinguishing it from conditions such as colonic diverticulitis, Meckel’s diverticulitis, and other gynecological pathologies in women, such as left ovarian disease, pelvic inflammatory disease, or a torsed/ruptured ovarian cyst, which may present as left-sided abdominal pain [1, 2].
In a normal individual, the appendix in the right iliac fossa results from a 270° counterclockwise rotation [9]. When the rotation occurs 270° clockwise, the appendix ends up positioned on the left side. A recent review of the literature reported 63 cases of situs inversus associated with left-sided appendicitis [10, 11]. This atypical localization often leads to diagnostic delays and increases the risk of severe complications. With the advent of modern imaging technologies, such as Doppler ultrasound and CT, which allow for the detection of such positional anomalies, the diagnosis can now be made earlier [12, 13].
Abdominal CT plays a pivotal role in guiding surgical management [12, 14], while laparoscopy is commonly considered the gold standard in these cases. It not only confirms the anatomical anomaly but also allows for appendectomy under laparoscopic guidance [15]. However, laparoscopy is technically more challenging due to the inverted view of abdominal organs in these patients, yet it remains indicated for both diagnosis and management of acute appendicitis in such cases.
Conclusion
Appendicitis is one of the most commonly observed abdominal surgical conditions, particularly in childhood, but also in adults. However, its atypical presentation in patients with situs inversus represents a significant diagnostic challenge, especially for those with no previous digestive history or who have never undergone a CT scan or ultrasound. This situation requires urgent and appropriate imaging, often based on CT, as well as a thorough understanding of the anatomical variations of the gastrointestinal tract. The management of this condition has been greatly improved with advancements in laparoscopic surgery, which is now further facilitated by progress in robotic surgery.
Author contributions
M.M. have written the article, have consulted the patient, and prepared the patient for surgery and participated in the surgery. S.Y. have helped writing the article, data collection. F.M. and H.B. have helped collecting data. G.A. and J.R. supervised the writing of manuscript. B.M. have supervised the writing of the paper, and has been the leader surgeon of the case.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}