





Abstract
Primary esophageal melanoma (PEM) is a rare and aggressive malignancy with limited treatment options. Due to its rarity, no standardized guidelines exist for managing oligometastatic recurrence, particularly in resource-limited settings. We present a case of a 60-year-old male with PEM who underwent esophagectomy followed by surgical resection of an adrenal metastasis. Despite the increasing use of immunotherapy, surgical resection remains a viable alternative for oligometastatic recurrence when access to systemic therapies is restricted. This case highlights the feasibility of surgery in achieving long-term disease control in select patients. Further studies are needed to establish evidence-based strategies for treating PEM recurrence in resource-constrained environments.
Introduction
Primary esophageal melanoma (PEM) is a rare malignancy, accounting for only 0.1%–0.5% of all esophageal cancers [1]. Its prognosis remains poor, with a median survival ranging from 3.7 to 34.5 months and a 3-year survival rate of 19% [2–5]. Due to its rarity, standardized treatment guidelines are lacking, with most available data derived from small-scale studies and case reports. Current therapeutic strategies include surgery, chemotherapy, and immunotherapy, though outcomes remain unpredictable.
Managing recurrent PEM presents an even greater challenge due to the scarcity of clinical evidence. While nivolumab has been successfully used in a few reported cases, including for recurrence, its clinical application remains limited [6–9]. Key challenges include its dependence on programmed death-ligand 1 (PD-L1) expression and restricted accessibility in low- and middle-income regions.
Case report
A 60-year-old male underwent screening in April 2021 due to complaints of dysphagia. His medical history was significant only for hip arthroplasty due to osteoporosis in July 2013, complicated by a recurrent chronic synovial-cutaneous fistula. Esophagogastroscopy revealed an elevated, white-colored tumor in the middle-lower thoracic esophagus, lacking visible black pigmentation. Histopathological analysis of the biopsy indicated an undifferentiated pleomorphic tumor, prompting immunohistochemical testing, which confirmed a spindle-cell, pigment-free malignant melanoma. The patient was referred to our hospital for further evaluation and management.
Chest and abdominal computed tomography (CT) revealed esophageal wall thickening (Fig. 1) without evidence of lymph node involvement or distant metastases. Laboratory tests, including tumor markers, were within normal ranges. A comprehensive dermatological evaluation found no signs of cutaneous melanoma or pigmented lesions. Based on these findings, the patient was diagnosed with clinical T3N0M0 primary esophageal melanoma according to the 8th edition of the Union for International Cancer Control (UICC) classification, though specific staging guidelines for this rare entity remain undefined.
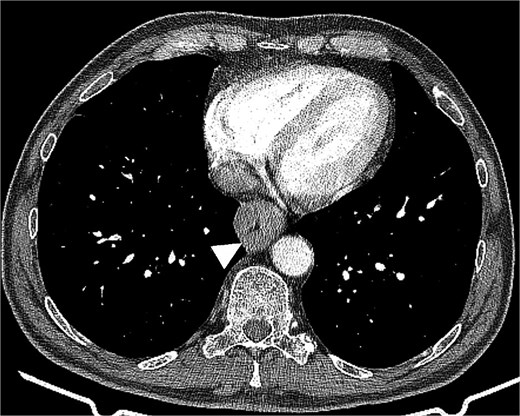
Chest computed tomography revealed esophageal wall thickening up to 31 mm, resulting in significant luminal stenosis.
Following a multidisciplinary team discussion, the patient underwent a hybrid esophagectomy (laparoscopy and thoracotomy) with two-field lymphadenectomy and gastric tube reconstruction via the posterior mediastinum in May 2021. The surgery lasted 310 min, with a total blood loss of 121 mL. Postoperatively, soft tissue inflammation around the jejunostomy tube was successfully managed with local therapy, and the patient was discharged 14 days after surgery.
The resected specimen measured 70 × 35 mm and appeared as an elevated, unpigmented, pinkish-white tumor (Fig. 2). Despite the initial histological findings of unpigmented melanoma, postoperative histopathological examination revealed pigment deposits, confirming a pigmented spindle-cell melanoma with lymphovascular (LVI1) and perineural invasion (PNI1) (Fig. 3). The surgical margins were clear (R0), and no lymph node involvement was detected, resulting in a pathological stage of pT3N0 (UICC, 8th edition) [8].

Macroscopic findings of the resected specimen. Gross appearance of the resected esophageal specimen.
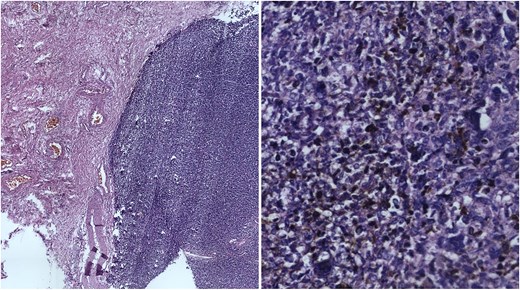
Microscopic findings of the resected specimen. Microscopic view (H&E) showing malignant pigmented spindle-cell melanoma with ulceration and necrosis.
In June 2022, 13 months after surgery, abdominal CT detected a 20.5-mm mass in the left adrenal gland extending toward the pancreatic tail (Fig. 4). Following multidisciplinary team evaluation, the patient underwent a laparoscopic left adrenalectomy, lasting 45 min, with an estimated blood loss of 80 mL. The tumor was completely resected, and the patient recovered without postoperative complications.
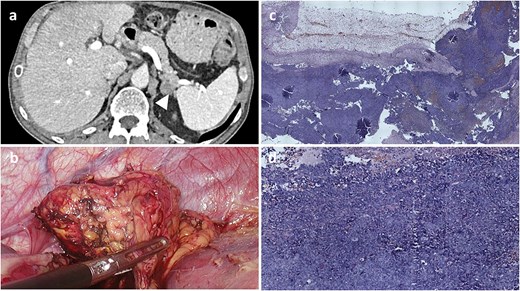
Radiological, intraoperative, and histopathological findings of adrenal metastasis. (a) Computed tomography revealing a 20.5-mm mass in the left adrenal gland extending toward the pancreatic tail. (b) Intraoperative view of the adrenal mass. (c and d) Microscopic examination (H&E) showing malignant pigmented melanoma within adrenal gland tissue.
Microscopic examination revealed a tumor composed of epithelioid cells with heterotypic nuclei, nuclear grooves, folding nuclei, intranuclear inclusions, and multinucleation (Fig. 3c). Immunohistochemical staining was negative for inhibin, synaptophysin, cytokeratin-pan, and chromogranin A, while vimentin and melanocytic markers (S-100, human melanoma black-45) were strongly positive, confirming metastatic melanoma.
In January 2025, 20 months after recurrence follow-up CT imaging showed no evidence of disease progression.
Discussion
Primary esophageal melanoma (PEM) is an extremely rare malignancy with a poor prognosis. The literature highlights the challenges in diagnosing PEM preoperatively due to its non-specific presentation and the frequent absence of melanin pigmentation. Misdiagnosis as squamous cell carcinoma is common, requiring careful histopathological and immunohistochemical assessment for accurate identification [6, 8].
The treatment landscape for PEM remains undefined due to its rarity. Surgical resection has traditionally been the primary approach, though its effectiveness in improving survival is uncertain. Some reports suggest that radical esophagectomy may offer a survival benefit in select cases, especially in the absence of distant metastases. However, the high recurrence rate, often within the first 2 years postoperatively, underscores the need for effective adjuvant therapies [10–12].
Recent advances in immunotherapy have shown promise in melanoma treatment, with anti-PD-1 agents such as nivolumab emerging as a viable option for PEM. Case studies, including the one presented here, suggest that nivolumab may play a critical role in controlling recurrence, particularly in metastatic settings. However, the availability and cost of immunotherapy remain significant barriers in many regions [6–9, 13, 14].
The long-term efficacy of immunotherapy in PEM remains to be fully established, with only limited data available. Future studies should focus on identifying biomarkers predictive of response to immune checkpoint inhibitors and exploring combination strategies with surgery and chemotherapy to improve outcomes. Given the aggressive nature of PEM, a multidisciplinary approach incorporating surgical, systemic, and supportive care is essential for optimal patient management.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}