





Abstract
Small bowel obstruction (SBO) is a common cause of acute abdominal pain, typically resulting from adhesions, hernias, or malignancy. Appendicitis is a rare etiology of mechanical SBO, with less than 50 cases documented in the literature. We report the case of a 66-year-old woman who presented with severe abdominal pain and vomiting. Computed tomography imaging revealed a closed-loop SBO with two transition points in the right lower quadrant and associated mesenteric congestion. Although the appendix appeared unremarkable on imaging, diagnostic laparoscopy identified an inflamed appendix forming a band encircling the small bowel, resulting in mechanical obstruction. A laparoscopic appendectomy was performed, with complete resolution of the obstruction. This case highlights a rare but important cause of SBO and emphasizes the role of early surgical intervention and diagnostic laparoscopy in identifying unusual intra-abdominal pathologies.
Introduction
Small bowel obstruction (SBO) is a common cause of acute abdominal pain and a frequent indication for surgical intervention, most often resulting from postoperative adhesions, hernias, or neoplasms [1]. Appendicitis, however, is an uncommon cause of mechanical SBO, with less than 50 cases reported in the literature over the past several decades [2]. The clinical presentation can closely mimic more common causes of SBO, making preoperative diagnosis particularly challenging. Imaging studies, particularly contrast-enhanced computed tomography (CT), may reveal transition points and mesenteric congestion, but the underlying role of the appendix is often only recognized intraoperatively. Due to the rarity of this condition, each reported case adds valuable insight into its pathophysiology, diagnosis, and surgical management.
We report a rare case of acute appendicitis causing a closed-loop SBO, diagnosed intraoperatively and successfully managed with laparoscopic appendectomy.
Case report
A 66-year-old woman presented to the emergency department with 12 hours history of severe, persistent abdominal pain. She reported multiple episodes of non-bilious, non-bloody vomiting and noted decreased passage of flatus. Her last bowel movement had occurred the day prior and was normal. She denied hematochezia, melena, or urinary symptoms. Her past surgical history was significant for a laparoscopic cholecystectomy and an open hysterectomy.
On physical examination, she was hemodynamically stable and afebrile. Her abdomen was distended, soft, and tender to palpation, particularly in the periumbilical region and right lower quadrant. Laboratory evaluation revealed leukocytosis with a white blood cell count of 16 × 109/L.
Contrast-enhanced CT of the abdomen and pelvis showed two closely positioned transition points in the right lower quadrant with moderate mesenteric congestion and interloop fluid. Those findings were suggestive of a closed-loop SBO (Fig. 1). The appendix was noted to be unremarkable in caliber but mildly stretched toward the transition point (Fig. 2). An enlarged paraesophageal hernia was also identified.
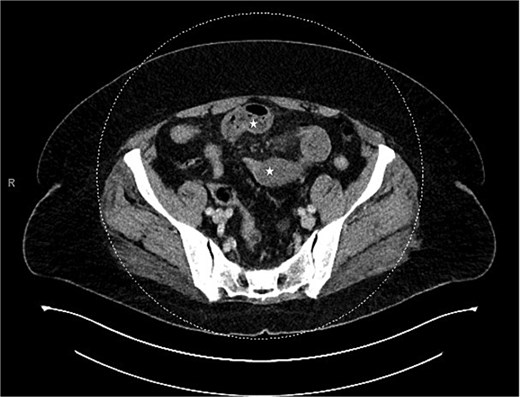
CT showing closed bowel loop obstruction and two closely positioned transition points.

CT showing the appendix (arrow).
Due to imaging findings and ongoing clinical concern for impending bowel compromise, the patient was taken to the operating room urgently and underwent a diagnostic laparoscopy. Intraoperatively, the appendix was found to be inflamed at the tip and it was adherent to the lateral abdominal wall (Fig. 3). The appendix was forming a band encircling a loop of small bowel, resulting in a mechanical obstruction (Fig. 4). Lysis of the adhesions was performed, successfully freeing both the appendix and the entrapped segment of small bowel (Fig. 5). The involved bowel segment appeared hemorrhagic but was not frankly ischemic, therefore bowel resection was not needed. A laparoscopic appendectomy was subsequently performed. The excised appendix measured 7 cm in length (Fig. 6). The obstruction was resolved, and the patient tolerated the procedure well. She had an uncomplicated postoperative recovery. She started passing gas and tolerated oral intake on postoperative day 1. She was discharged on postoperative day 2. At her follow-up clinic visit, her incisions were well-healed. She reported normal bowel function, no abdominal pain, and was gradually resuming her regular activities. Overall, she was recovering well, with no concerns.
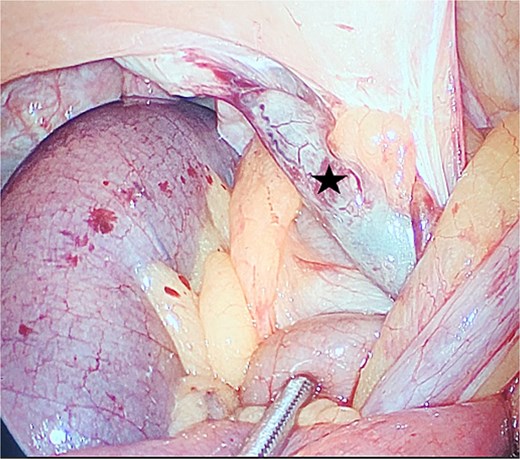
The appendix adherent to the lateral abdominal wall (star).
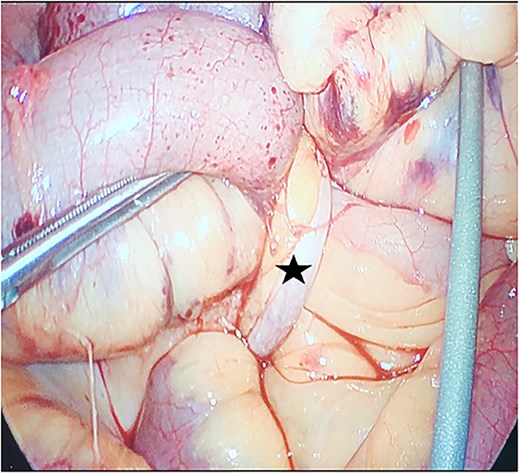
The appendix forming a band around the small bowel, causing small bowel obstruction (star).
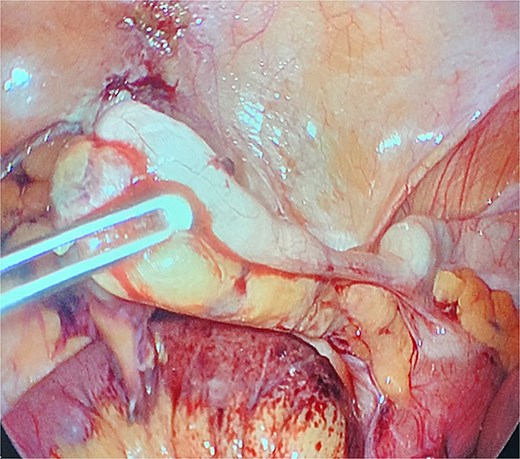
Freed appendix following lysis of adhesions.

Gross specimen of the excised appendix, measuring 7 cm in length.
Discussion
SBO is a common surgical emergency caused by mechanical or functional impairment of intestinal transit. It most frequently results from postoperative adhesions, with other causes including hernias, malignancies, and less common etiologies such as volvulus, gallstone ileus, or endometriosis [3]. Fewer than 50 cases have been published identifying acute appendicitis as the underlying cause [2]. Although appendicitis is one of the most frequent abdominal emergencies, its presentation as a cause of mechanical SBO is exceedingly rare.
Acute appendicitis typically results from luminal obstruction caused by fecaliths, lymphoid hyperplasia, or neoplasms, and may progress to perforation, abscess formation, or generalized peritonitis if left untreated [4]. In rare cases, however, it may lead to mechanical small bowel obstruction through several distinct mechanisms.
The first case of intestinal obstruction secondary to acute appendicitis was described by Hotchkiss in 1901 [5]. Appendicitis-induced SBO can result from a variety of mechanisms. Adynamic obstruction (paralytic ileus) is the most common, arising from the inflammatory spread to adjacent structures such as the cecum, small bowel, or posterior peritoneum. Adhesions or inflammatory bands may also form between the appendix and adjacent bowel or peritoneal structures, causing kinking or entrapment of small bowel loops. In some cases, the appendix forms a fibrous or inflammatory band encircling a loop of bowel, referred to as appendiceal tie syndrome, leading to a closed-loop obstruction with the potential for strangulation and ischemia. Only a handful of cases have described a loop of appendix adherent to the abdominal wall, resulting in closed-loop obstruction, similar to the presentation observed in our patient [6].
Although imaging did not reveal overt signs of appendiceal inflammation, the appendix was stretched toward the site of obstruction, highlighting the importance of intraoperative exploration when clinical suspicion for a mechanical cause remains high. Prompt surgical intervention is essential in such cases to prevent bowel ischemia and necrosis. Diagnostic laparoscopy serves both diagnostic and therapeutic purposes, and laparoscopic appendectomy with lysis of adhesions remains an effective and minimally invasive treatment strategy, offering favorable outcomes when diagnosis is made early.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}