





Abstract
Peptic ulcer perforations are common in surgical emergencies, whereas double perforations are rare, and triple peptic perforations are even exceedingly rare, with only a few cases documented. While undetected perforation during surgery can be fatal, the absence of standardized procedures for managing multiple perforations remains an ongoing challenge for surgeons. Herein, we describe a rare case of simultaneous triple peptic perforations in an elderly man with a prolonged history of analgesic and corticosteroid use. This case underscores the importance of screening multiple peptic perforations intraoperatively. Subtotal gastrectomy is suggested as an effective option when simple closure of perforations is infeasible.
Introduction
Peptic ulcer disease (PUD) affects approximately four million people worldwide annually, with an incidence of 1.5%–3% [1, 2]. Although PUD can be managed with medications, perforated peptic ulcer remains as a severe complication with a high mortality risk. Approximately 2%–14% cases with PUD were reported to involve perforation, particularly in elderly patients [2, 3]. Signs and symptoms of perforation include sudden abdominal pain, tachycardia, and rigidity, and plain radiography with free air under the diaphragm as a diagnostic sign [2, 4, 5]. Patients with perforation can develop peritonitis with acute abdomen and high risk of morbidity and mortality [6, 7]. Among various factors responsible for increasing gastric acid secretion, nonsteroidal anti-inflammatory drug (NSAID) treatment, high salt intake, and Helicobacter pylori infection are reported as primary risk factors causing gastric ulcer and associated perforation [4, 7, 8].
It is uncommon for patients to present with double peptic perforations, while triple perforations are incredibly rare, with only a few cases reported [4, 9–11]. While there is no consensus in managing multiple gastric perforations, these cases raised substantial concerns for surgeons handling complicated cases. Here, we report an exceptionally rare case of synchronous triple peptic perforations in an elderly male with a history of using NSAID and corticosteroid for more than 3 months.
Case presentation
A 74-year-old man was admitted to the emergency department with severe, unremitting abdominal pain. Physical examination revealed guarding and rigidity. Plain abdominal X-rays revealed free gas under both hemi-diaphragms (Fig. 1). His medical history recorded arthritis, for which he has been treated with NSAID and corticosteroids for over 3 months. An indication of emergency laparotomy was performed for the patient with an initial diagnosis of generalized peritonitis due to gastrointestinal perforation.

X-ray showing free air under both hemi-diaphragms, indicative of gastrointestinal perforation.
Through intraoperative laparotomic exploration, surgeons discovered three distinct perforations: two perforations in the first part of duodenum with sizes of 0.5 and 1.5 cm, respectively, and another 1 cm perforation in the prepyloric region (Fig. 2). The peritoneal cavity was irrigated with 3 l of normal saline, and biopsies of the ulcer margins were taken. As simple suturing of the perforations was not feasible, a subtotal gastrectomy with a Roux-en-Y reconstruction was performed. The patient fully recovered and was discharged on the ninth postoperative day. Postoperative barium gastrography 1 month later confirmed normal flow at the gastrojejunal anastomosis (Fig. 3).
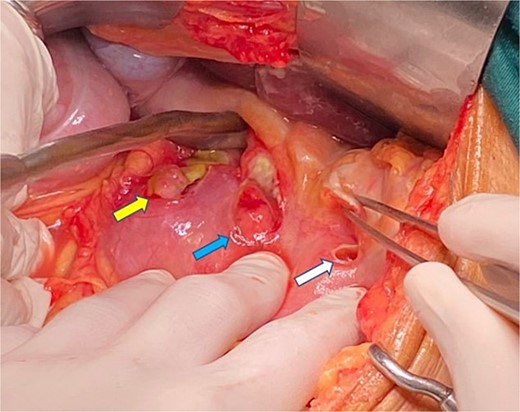
Intraoperative photograph demonstrating triple gastric perforations (yellow, blue, and white arrows indicate the locations of the perforations).

Postoperative barium gastrography revealing good flow at the gastrojejunal anastomosis.
Discussion
Peptic ulcer perforation remains a prevalent surgical emergency with significant morbidity and mortality, particularly among elderly patients [6, 7]. Clinical symptoms and signs of peptic perforation can be various amongst patients, but this case illustrated typical symptoms with sudden onset of abdominal pain with guarding and rigidity. The X-ray image of free air under both hemi-diaphragm reenforced the diagnosis.
Perforations occur most frequently in the duodenum (35%–65%), followed by the pylorus (25%–45%) and stomach (5%–25%) [12]. Most cases of multiple peptic ulcer perforations were found with two perforations [4, 9, 11]. The only other reported case of triple gastric perforations was described by Radojkovic et al. [10] in a 41-year-old female on anticancer drugs. Key etiological factors include H. pylori infection and prolonged NSAID or corticosteroid use, with incidence varying by sociodemographic factors [7, 8]. In this case, it is possible that prolonged usage of NSAID and corticosteroid in the old patient contributed as a main cause to the development of peptic perforations. However, there is no evidence suggesting triple peptic perforation before surgery. It is crucial for surgeons to thoroughly investigate every possible perforation intraoperatively. Therefore, further study to identify high risk of multiple peptic perforations in patients is essential.
Standard management of peptic perforations typically involves primary closure, suitable for single or double perforations [2–4]. However, when simple closure is impractical in cases with multiple or complex perforations, subtotal gastrectomy is recommended as a more reliable alternative to ensure complete removal of damaged tissue and prevent leakage [10, 11]. This standing report demonstrates that subtotal gastrectomy can effectively manage multiple perforations, leading to control of symptoms and a decrease in recurrence risk, especially in elderly patients with prolonged NSAID or corticosteroid use.
Conclusion
Simultaneous triple peptic perforations are exceptionally rare and can be life-threatening if they are left undetected during surgery. Surgeons should be mindful of the possibility of multiple perforations, especially in high-risk patients with prolonged NSAID or corticosteroid use. When simple closure of multiple perforations might be complex and risky of postoperative complications, subtotal gastrectomy could be an effective approach for addressing multiple peptic perforations.
Acknowledgements
We thank Can Tho University of Medicine and Pharmacy for the support.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
No financial support was provided for the study.

{kind=link}
{kind=link}
{kind=link}