





Abstract
Mantle cell lymphoma (MCL), representing 5% of cases, is an aggressive B-cell non-Hodgkin lymphoma. Rarely, it can spread to other areas. This case illustrates a unique occurrence of MCL involving the appendix, leading to obstructive symptoms. Additionally, its presentation as volvulus added complexity to diagnosis and treatment. A 72-year-old man with a history of MCL came to the ER with right lower quadrant abdominal pain and nausea for 7 days. A computed tomography scan showed a swirling sign, concerning for volvulus. The patient required emergent surgery for exploratory laparotomy. Intraoperatively, the patient was found to have an enlarged appendix measuring 16.5 cm in length and 5 cm in diameter. An appendectomy was performed, and the pathology was confirmed to be MCL. This is a rare case of MCL presenting in the appendix as a volvulus, resulting in obstructive symptoms. This distinctive manifestation posed significant challenges in diagnosis and management. Appreciating such cases is pivotal for accurate diagnosis and effective medical and surgical interventions for this aggressive lymphoma subtype.
Introduction
Mantle cell lymphoma (MCL) is a rare subtype within the domain of B-cell non-Hodgkin lymphoma (NHL) with an annual incidence of only one case per 200 000 individuals [1, 2]. Within the broader spectrum of NHLs, MCL represents a modest 5%; however, its aggressive nature is notably conspicuous.
Survival statistics within the realm of MCL delineate a median overall survival (OS) ranging from 5 to 7 years [3]. However, the prognosis for individuals who have relapsed or refractory MCL takes on an even graver character, with a median OS curtailed to a mere 6–10 months [3].
MCL typically inaugurates its clinical journey with the enlargement of lymph nodes; however, its proclivity for dissemination to diverse anatomical precincts, including the bone marrow and liver, is an established facet of its clinical course. However, the extension of the MCL to the appendix represents an exceedingly rare occurrence, warranting meticulous attention. The case report in question reveals an exceptional scenario, chronicling a patient’s recurrent struggle with MCL that surfaced in the form of an enlarged appendix.
Case presentation
A 72-year-old male, who had previously been diagnosed with MCL in 2021 and had undergone R-CHOP therapy achieving remission, presented to the Emergency Department with a history of right lower quadrant abdominal pain, lightheadedness, and persistent nausea for over a week. Upon initial evaluation, computed tomography (CT) (Fig. 1) raised the suspicion of a potential volvulus. However, upon transfer to the operating room, a markedly distended appendix, accompanied by substantial lymphadenopathy affecting the mesoappendix, was unveiled (Figs 3–5). An appendectomy was subsequently performed, and the excised specimen was promptly dispatched for pathological examination, which confirmed the presence of MCL.

An image of the mass (pointing arrow) on (a) axial view showing Swerling sign, (b) coronal view.
Remarkably, during surgery, several lymph nodes and a small mass causing bowel obstruction were found. The mass was resected, and the intestine was re-anastomosed. Pathological analysis confirmed the mass as MCL.
The patient developed an elevated white blood cell count of over 114 000, raising concerns about MCL recurrence. Fortunately, no further incidents occurred, and the patient was discharged with follow-up scheduled with both the general surgery team and the oncologist.
Discussion
MCL is a rare type of B-cell NHL with a median OS of 5 to 7 years, dropping to 6 to 10 months in refractory cases [2]. Characterized by t(11;14)(q13;q32) translocation and cyclin D1 overexpression, MCL’s clinical course varies widely, presenting as either aggressive or indolent. No curative treatments exist, and relapsed MCL remains challenging to manage [3].
MCL often starts with lymph node enlargement and can spread to the bone marrow, liver, and gastrointestinal tract, especially the colon. It rarely affects the appendix, typically through nearby ileocecal involvement [4, 5]. In our case, a 1.4 cm appendiceal mass was found on a positron emission tomography CT (PET-CT) scan a year prior to presenting with the symptoms, but follow-up was not pursued until the patient presented with pain and obstructive symptoms due to an enlarged appendix, confirmed by CT to be a “swirl sign” indicative of volvulus (Figs 1 and 2). The appendix measured 5 cm in width and 16.5 cm in length (Figs 3–5).
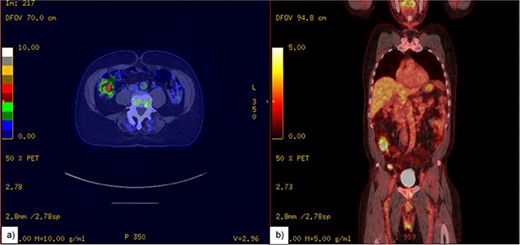
A PET-CT scan of appendix. (a) Thickening of the appendix measuring up to 1.4 cm with increased Fluorodeoxyglucose (FDG) avidity. (b) Showing appendix in coronal view.

Intraoperative findings of small bowels and the appendix.

Intraoperative image of the appendix.
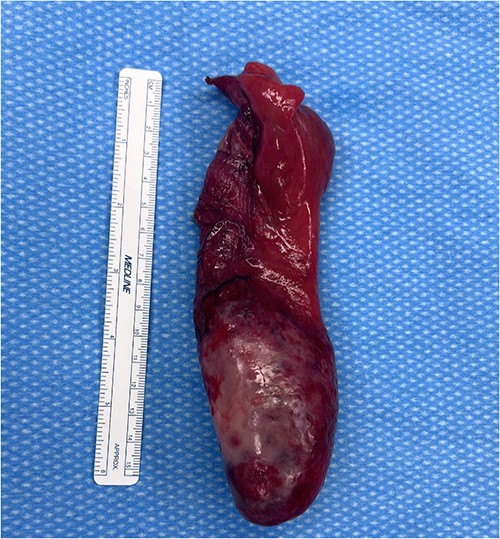
Appendix with a ruler next to it, measures ~17 cm in length and 5 cm in diameter.
Surgical management lacks a standard protocol, with right hemicolectomy or single appendectomy being common. Our patient underwent an appendectomy, small bowel resection, and primary anastomosis. The long-term outcomes of such surgeries are unclear, emphasizing the need for more case reports to guide management. Reporting rare MCL cases, especially those involving the appendix, is essential for improving recognition and treatment strategies.
Conclusion
We report a rare case of MCL in the appendix, where the patient was presented with abdominal pain and a distinct “swirl sign” on a CT scan. The appendix was significantly enlarged, measuring 5 cm wide and 16.5 cm long, leading to appendiceal torsion. This is the first documented instance of MCL causing appendiceal volvulus with a swirl sign on CT. The rarity of this presentation, along with vague symptoms, caused a diagnostic delay. This highlights the need for more understanding and documentation of such cases to improve diagnosis and treatment. Managing MCL in the appendix differs from other lymphomas in this area.
Conflict of interest statement
None declared.
Funding
None declared.
Consent
Consent for the study was obtained by all involved participants in the study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}