





Abstract
Retrocaval ureter is a rare congenital vascular anomaly with an incidence of 0.13%, leading to the passage of the right ureter behind the inferior vena cava and then turning around it to attain its lateral position. The condition is usually associated with obstruction in the right kidney and proximal ureter leading to symptoms like dull aching pain in the flanks, recurrent episodes of urinary tract infections, and recurrent stone formation. The patient presented with recurrent episodes of burning micturition and pain in the right flank for the past 6 months. A contrast-enhanced computed tomography kidney–ureter–bladder was done to diagnose the condition. The patient was managed by open pelviureteric anastomosis lateral to the inferior vena cava, thus eliminating the obstruction on the ureter. The patient has had an uneventful postoperative follow-up. Retrocaval ureter is a rare condition and should be clinically suspected in cases of hydronephrosis where other causes have been ruled out. Different approaches can be used to correct the anomaly. In this case report, an open transperitoneal intraabdominal approach has been used.
Introduction
The retrocaval ureter is a rare congenital anomaly resulting from the abnormal development of the inferior vena cava (IVC). The right posterior cardinal vein normally lies lateral to the definitive ureteral position. When the right subcardinal vein persists as the renal segment of the IVC, a retrocaval or circumcaval ureter results [1].
A meta-analysis of 13 studies on retrocaval ureters concluded that the prevalence of the condition is 0.13%. Even if present, retrocaval ureter rarely causes symptoms, primarily due to the development of hydroureteronephrosis (HUN) [2].
Although it is a congenital anomaly, patients usually present in the third or fourth decades of life with dull aching pain in the flank due to the associated HUN [3].
We present here a case of a 26-year-old male with a retrocaval ureter, presenting as pain in the right flank region.
Case presentation
A 26-year-old male presented to the Urology outpatient clinic with complaints of pain in the right flank and intermittent episodes of burning micturition for the past 6 months. For these symptoms, he received multiple short courses of antibiotics. There was no significant surgical history. There were no history of hematuria, palpable lump, fever, or dysuria. On examination of the abdomen, there was mild tenderness in the right flank but no lump was palpable. Rest of the systematic examination was normal.
Routine investigations were done, which showed a haemoglobin of 10.2 g/dl, white blood cell count of 6500/ mm3, urea of 7 mg/dl, and creatinine of 0.5 mg/dl. Urine analysis showed 2–3 RBCs/High Power Field and 10–12 WBCs/High Power Field.
An abdominal ultrasound was done, which revealed moderate right-sided hydronephrosis and proximal dilated ureter. A routine X-ray kidney–ureter–bladder (KUB) showed no obvious radio opaque shadow in the renal pelvis. A contrast-enhanced computed tomography (CECT) KUB was done, which showed moderate right Hydroureteronephrosis (Fig. 1) extending to the proximal ureter with papillary necrosis, consistent with retrocaval ureter (Fig. 2).
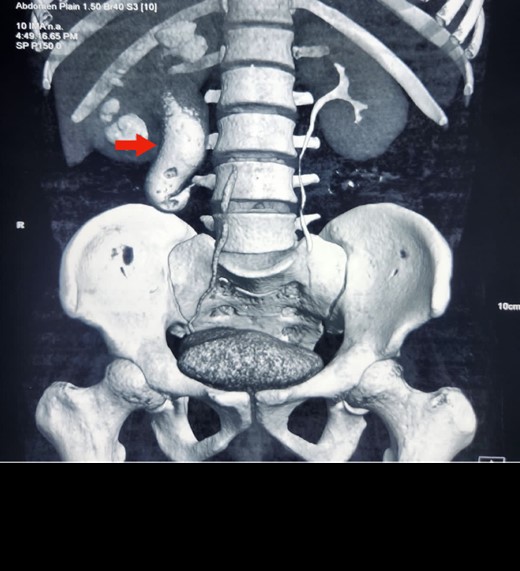
Reconstruction image of CECT KUB showing retrocaval ureter (arrow) and hydronephrosis of right kidney with dilated proximal ureter.

CECT KUB image showing gross right hydronephrosis (arrow).
The patient was planned for surgery because of the symptoms after taking informed consent.
A midline incision was given, and the abdomen was opened from 4 cm below the xiphisternum to 3 cm above the pubic symphysis. The ascending colon along with the hepatic flexure was completely mobilized medially to expose the retroperitoneum. Careful dissection was done to identify the IVC and its the relations to the right ureter. The proximal dilated ureter and right pelvicalyceal system were identified, and dissection was continued laterally. The ureter was traced and noticed to course behind the IVC at the level of the L2–L3 vertebra, exiting to lie medially in the groove between the IVC and the aorta (Fig. 3). The ureter was divided proximal to the point where it coursed behind the IVC until it came out medial to IVC (Fig. 4). The retrocaval segment was brought anteriorly, resected from the normal distal ureter, and ureteropelvic anastomosis was done using 3–0 Polyglactin sutures lateral to the IVC (Fig. 5). This procedure eliminated the compression on the ureter. An abdominal drain was placed.
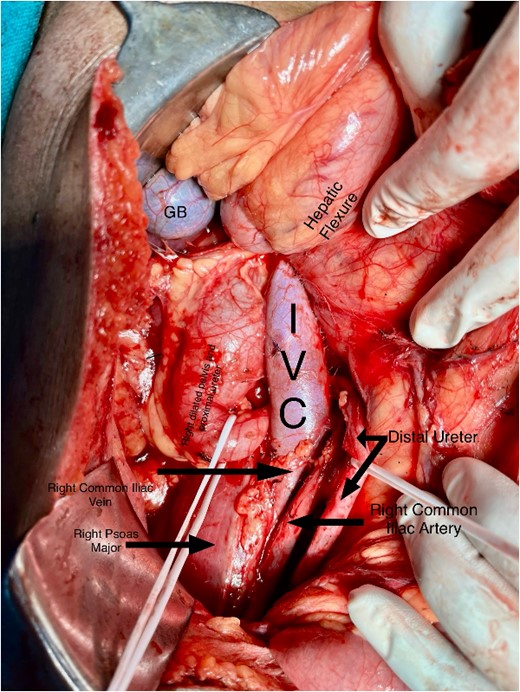
Intraoperative image showing the course of the retrocaval ureter and the important structures around it.
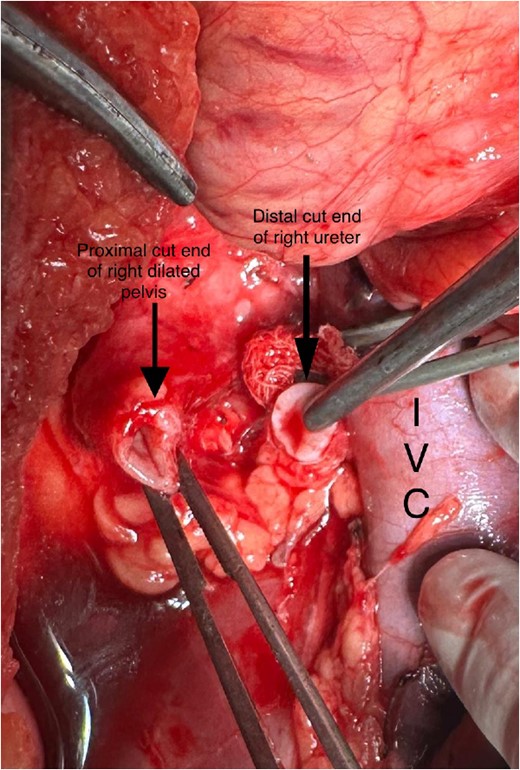
Intraoperative image showing cut end of the ureter.
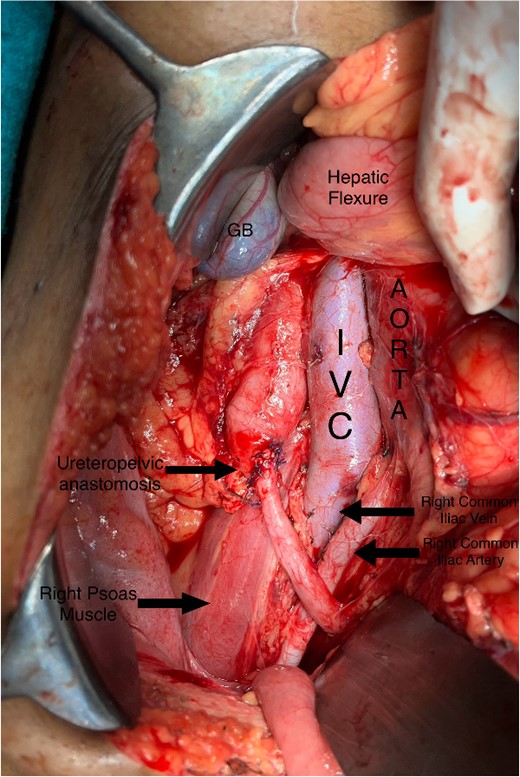
Intraoperative image showing pelviureteric anastomosis after resection of retrocaval part of the ureteric segment.
Postoperative period was uneventful, and the patient was discharged on postoperative day 3 under stable conditions.
Discussion
Retrocaval ureter is a rare congenital anomaly that results by an abnormal formation of infrarenal IVC from anteriorly located subcardinal vein, resulting in ureter passing posteriorly to the IVC [1].
Qureshi MA, Mulvaney WP found it is three times more common in men than in women [4].
Kyei MY, Yeboah ED, Klufio GO, et al reported that retrocaval ureter has been divided into two clinical types: Type 1, also called low loop, is characterized by the typical fishhook deformity of the ureter, at the level of L2–L3; Type 2 with less medial deviation of the ureter with mild or no symptoms with Type 1 being more common [5]. In our case, the patient had Type 1 or low type retrocaval ureter.
de Arruda GJF, de Arruda Neto JF, et al found that patients usually present with symptoms of dull aching pain, recurrent UTI, and nephrolithiasis in the third or fourth decade of life [6]. In our case, the patient had similar clinical presentation.
Imaging studies are important for definitive diagnosis of the rare condition. Abdominal ultrasound reveals hydronephrosis and proximal hydroureter. CECT KUB is the diagnostic modality of choice [2]. In our case, a CECT KUB was done, which confirmed the diagnosis of retrocaval ureter with right-sided HUN.
Qureshi MA, Mulvaney WP advised that surgery is required in patients with persistent symptoms or worsening of renal function. The standard repair is open surgical pyelopyelostomy or ureteroureterostomy. Repair usually includes resection of redundant retrocaval ureteral segment, anteposition, and anastomosis [4]. In our case, we also followed the same surgical principles to preserve the renal function.
Conclusion
Retrocaval ureter is a rare congenital anomaly resulting from the persistence of the right subcardinal vein. Patients usually present in the third or fourth decade with pain in the right flank, recurrent episodes of urinary tract infection, and stone formation. CECT KUB is the investigation of choice to diagnose the rare condition. Ureteroureterostomy or pelvi ureterostomy is the recommended treatment of choice.
Author contributions
Manzoor Ahmad: Part of the surgical team.
Ezaz Ahmed: Part of the surgical team.
Wasif Mohammed Ali: Concept for the case report.
Saifullah Khalid: Consultant Radiologist.
Imad Ali: Part of the surgical team.
Conflict of interest statement
The authors declare that they have no competing interests.
Funding
No funding procured.
Data availability
The information generated during the case report is included in this published article and is available for review.
Ethics approval and consent to participate
This work is exempted from ethical approval in our institution because of its type.
Consent for publication
Written informed consent was obtained from the patients for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}