





Abstract
The most frequent benign tumor is lipoma. About 1–4% of people have intraoral lipomas. This uncommon case report shows a large cheek lipoma misinterpreted as dental infection. A 14-year-old girl with a right cheek tumor was diagnosed and treated for a dental infection. Multiple imaging examinations complete the diagnosis. A benign lipoma, common in subcutaneous tissues but unusual in the mouth, created the lesion. A histological investigation confirmed lipoma after extraoral excision under general anesthesia utilizing an external flap. The edema did not return after surgery, which restored face symmetry. This case study shows that diagnosing and treating oral and maxillofacial edema requires extensive clinical and radiographic testing. Lipomas should be evaluated in the differential diagnosis of mouth swelling even without usual risk markers to prevent excessive treatments and delays. Surgery is recommended for lipomas since it has a low recurrence and fewer risks.
Introduction
Lipoma is considered the most prevalent benign tumor compared to other benign neoplasms, with a prevalence of 2.1 per hundred people, and it is known to be a universal tumor as it can develop in any location in the body [1]. It is mostly located on the trunk and extremities [2]. However, it represents 0.1–5% of all benign tumors of the mouth, usually found as long-standing soft nodular asymptomatic swellings covered by normal mucosa [1].
In 1948, Roux was the first person to formally characterize the condition known as oral lipoma. He referred to it as the “yellow epulis” [3] and was the first to use that name. Intraoral lipomas have a very low incidence rate, ranging from 1 to 4%. This finding was further reinforced by a study conducted by Furlong et al. [4]. In this investigation, scientists discovered 125 oral lipomas over the course of 20 years. Although it is uncommon for a lipoma to occur in the oral cavity, if it does, it might occur mostly in the buccal mucosa, tongue, and mouth floor [4]. It may present as a solitary mass or multiple masses. These adipocyte tumors are typically asymptomatic and are discovered incidentally on radiography. The etiology and pathogenesis of lipomas remain unclear, although mechanical trauma, endocrine disorders, obesity, hypercholesterolemia, radiation, and chromosomal abnormalities have been reported [5]. Swelling and discomfort are sporadic symptoms in symptomatic cases [6].
The present case was diagnosed as a large cheek lipoma that was misdiagnosed and medically treated as a dental infection for 2 years.
Case presentation
A 14-year-old unmarried female student was referred to the Oral and Maxillofacial Department of the Hospital. Upon receiving this patient for her first visit, she complained of swelling in her right cheek for 2 years, which continued to increase in size, leading to discomfort and difficulty during chewing and swallowing. Previously, it was regarded as a case of dental infection and was managed accordingly; however, it never became a cure. The patient had no history of mechanical irritation or trauma from sharp teeth. The patient had a history of taking inappropriate analgesics and antibiotics and had no sensitivity to any known medication. The patient had no family history of the same condition, smoking, or alcohol consumption.
A clinical intraoral examination demonstrated normal oral tissues and salivary flow from all major salivary glands. There was a huge smooth swelling on her right cheek that extended to the submandibular region. On palpation, the mass was painless, not tender, had no skin changes, had no dilated veins over the swelling, was lobulated, and the facial sensation was normal. It was slowly getting bigger, which bothered the patient because it looked bad and made her feel that negative fine-needle aspiration results were also observed.
Laboratory investigations included a full blood count that revealed a slightly lower MCV, MCH, and MCHC with slightly elevated platelets. Other laboratory investigations, including lipid profiles and blood sugar levels, were normal. As far as diagnostic assessment is concerned, the patient underwent several imaging examinations. Ultrasonography showed a 30 × 12 mm irregular cystic lesion in the right cheek with echogenic foci. For further characterization of the lesion, a computed tomography (CT) scan (IV contrast) showed a 44 × 42 mm fat-containing cystic lesion, which revealed periapical radiolucency associated with the lower right 2nd molar tooth, involving both roots. Doppler ultrasound of the neck also showed a well-encapsulated right cheek mass, a typical lipoma with no internal blood vessels, a vascular or lymphatic malformation, and a teratoma. These results confirmed the CT scan results. A contrast-enhanced magnetic resonance imaging (MRI) (Fig. 1) was performed to confirm the CT results. The decision to perform surgical extraoral excision was made under general anesthesia using the external flap approach, as in parotidectomy, after obtaining the patient’s and the family’s consent. The skin and subcutaneous layers were reflected during the procedure using the external flap approach (Fig. 2). After exposing the facial nerve and its branches and looking at them, the 20 cm lipoma was cut out between the nerve’s branches (Fig. 3), and all other structures were stitched back together. The specimen was sent for histopathological examination. The gross surgical specimen was a multilobulated, yellowish, encapsulated mass ~20 cm long. Hematoxylin and Eosin (H&E) staining of microscopic sections of the specimen revealed sheets of mature fat cells in a characteristic lobular structure with a thin fibrous capsule. In large, ovoid to polygonal cells, adipocytes have an eccentric nucleus pressed against the cytoplasmic membrane, a transparent cytoplasm, and a cytoplasmic membrane. The final diagnosis of lipoma was confirmed.
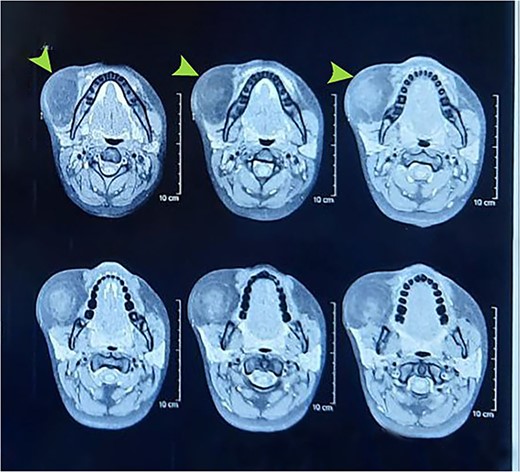
Preoperative MRI showing right cheek mass.
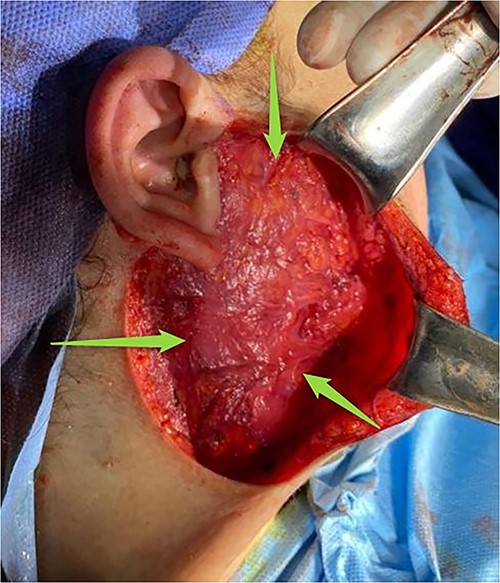
During operation.

Surgical specimens measuring 20 cm.
The patient received a ceftriaxone vial (1 × 2) for 4 days postoperatively. Paracetamol ampule 600 mg (1 × 1) for 4 days. Topical skin gel to accelerate the healing process. During the following months, no complications or recurrence of swelling were noted (Fig. 4), the normal shape and symmetry of the face were restored, and the patient was comfortable with no pain or deformity.
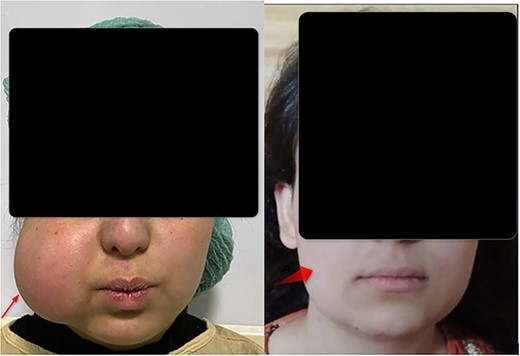
(A) Preoperative right cheek lipoma. (B) Postoperative after 6 months follow up.
Discussion
This report presents a rare case of a large cheek lipoma that was misdiagnosed and medically treated as a dental infection for 2 years. Lipomas are often asymptomatic; however, they may present with symptoms associated with their size or location. These symptoms may lead to functional impairment or esthetic problems. Clinically, these tumors manifest as lumps under the skin or mucosa with a normal appearance, are soft, do not cause discomfort, and can be moved. However, because lipomas are uncommon in the oral and maxillofacial areas, they may be difficult to diagnose, which can lead to incorrect diagnosis and improper treatment [7].
Lipomas are the most common benign tumors, typically found in the subcutaneous tissues of the trunk and extremities [8]. However, they can occur at any location in the body, including the oral cavity, and oral lipomas are relatively uncommon owing to the scarcity of fat in this region [9]. Few studies have demonstrated equal sex distribution for the tumor [4], while others have shown a slight male predilection [10]. The present study showed a female preponderance. The excised material in the current study measured ~20 cm in length, which is a significant size. This is probably attributable to the fact that the diagnosis was delayed for 2 years. When the patient first observed the lipoma and decided to seek medical assistance, the time span varied from 1 month to 10 years (the mean was 2 years) [11].
Lipomas are frequently associated with mechanical trauma, endocrine disorders, obesity, hypercholesterolemia, radiation exposure, chromosomal abnormalities, and diabetes mellitus. However, its precise etiology and pathogenesis remain unknown [12]. On the other hand, the patient in this instance did not have any previous history of mechanical irritation or harm caused by sharp teeth, yet she was incorrectly diagnosed with a dental infection. In this case, histopathological analysis showed that the mature adipocytes were set up in distinct lobulated structures and surrounded by a thin fibrous capsule. These cells, varying from ovoid to polygonal in shape, displayed an eccentric nucleus abutting the cytoplasmic membrane and a clear, transparent cytoplasm. Interestingly, they were morphologically indistinguishable from typical fat cells, with the only distinguishing feature being an enclosed thin fibrous capsule. Imaging is a crucial part of the diagnostic process whenever a lipoma is believed to be present. Ultrasound, CT, and MRI are some of the helpful imaging modalities [13].
Given the striking resemblance between the histological characteristics of lipomas and normal adipose tissue, it is imperative to consider other tumor-like conditions in the differential diagnosis. These include epidermoid cysts, pleomorphic adenomas, fibromas, thyroglossal duct cysts, ectopic thyrohyoid tissue, mucoepidermoid carcinoma, oral dermoid, and lymphoepithelial cysts [3, 12]. The treatment of choice for lipoma is surgical excision; however, removal can be challenging if the tumor is located deep [14]. Recurrence or complications are uncommon following surgical excision.
Conclusion
This case report describes an uncommon big cheek lipoma that was misdiagnosed as a dental infection for 2 years. Despite being the most prevalent benign tumor, lipomas of the oral cavity are rare. Even without risk factors, such as mechanical trauma or endocrine problems, lipomas should be included in the differential diagnosis of oral and maxillofacial swelling. Surgery is the preferred treatment for lipomas that rarely recur. Clinical and radiological assessments must be performed to minimize misdiagnosis and treatment delays.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}