





Abstract
Trocar site hernia is a rare, serious operation-related complication after robotic gynecologic surgery. Here, we present two 8-mm port-site hernia cases after three-port robotic myomectomy with a review of reported previous cases. In the first case, small bowel obstruction was found postoperatively due to herniation at the left mid-axillary line 8-mm trocar site. Small bowel herniation through the same site as the first case was found in the second case. Emergency exploration was performed in both cases by extending the left trocar site. There was no sign of bowel ischemia, and successful bowel reduction and hernia repair were done. Unlike previously reported cases, these cases occurred in a normal body mass index (BMI) patient (first case 20.28 kg/m2, second case BMI 24.80 kg/m2) and were pelvic drain insertion sites. These sites were the weak points of the abdominal muscle coverage. Therefore, the closure of 8-mm trocar sites should be considered.
Introduction
Trocar site hernia (TSH) is defined as developing a hernia at the port insertion site after laparoscopic or robotic surgery. In laparoscopy, the frequency of herniation in ports <10 mm was up to 0.09% [1].
Although most trocar sites in robotic procedures are <10 mm, it is essential to recognize that some hernia cases are accompanied by an intestinal obstruction that requires emergent surgery. Here, we report two 8-mm port site hernia cases in the three-port robotic myomectomy (3PRM), followed by a review of previous hernia cases in gynecologic robotic surgeries.
Case description
Case 1
A 38-year-old woman with a huge myoma measuring 12 cm in diameter was admitted for 3PRM due to menorrhagia. Her body mass index (BMI) was 20.28 kg/m2. On 9 November 2020, she underwent a 3RPM with an umbilical single-port incision (1.5 cm) and two other 8-mm assistant ports on the left and right anterior axillary lines 8–9 cm apart from the umbilicus (Fig. 1). The surgery was performed with the Da Vinci Xi Surgical System (Intuitive Surgical, Sunnydale, CA, USA) without intraoperative complications. After the surgery, the 15-mm umbilical single-port site was closed with an interrupted absorbable suture layer by layer. A Jackson-Pratt (JP) drainage was inserted at the left port site.
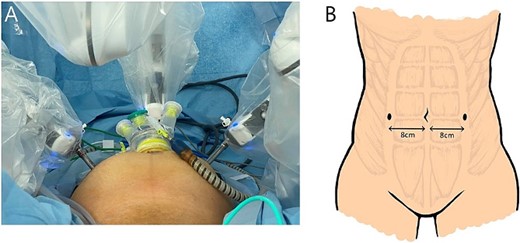
(A) The surgical setting of a 3PRM. (B) An anatomical illustration of 8-mm trocar sites in 3PRM.
On postoperative day (POD) #1, she complained of abdominal distension with mild nausea and vomiting. An abdomen X-ray showed air-fluid levels (Fig. 2A). Follow-up X-ray revealed aggravated ileus on POD#4 (Fig. 2B). An abdominal computed tomography (CT) scan demonstrated small bowel obstruction due to herniation at the left 8-mm port site (Fig. 2D), with the drain in situ. Emergency exploration showed that herniation occurred along with the left port site drain tract; however, there was no sign of bowel injury. Surgical repair was done, and the patient recovered well (Fig. 2C).
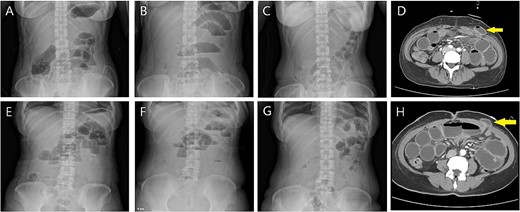
(A) Case 1: abdomen X-ray on POD #1; prominent small bowel gas with air-fluid level. (B) POD #4: aggravated ileus. (C) POD #7 after robotic myomectomy (POD #3 after exploration): recovered to a nonspecific normal gas pattern. (D) Small bowel herniation (arrow) is noticed at the left mid-axillary trocar site on a CT scan. (E) Case 2: abdomen X-ray on POD #3; mild ileus with air-fluid level (F) POD#6 on the morning of surgery: persistent ileus with L-tube in situ. (G) POD #9 after robotic myomectomy (POD #3 after exploration): nonspecific bowel gas shadow. (H) Small bowel herniation (arrow) is noticed at the left mid-axillary trocar site on a CT scan.
Case 2
A 51-year-old woman with multiple growing myomas visited our clinic with abdominal discomfort and frequent urination. Her BMI was 24.80 kg/m2. Imaging evaluation with magnetic resonance imaging and ultrasonography revealed multiple myomas, with the largest diameter of 12.3 cm. She underwent 3RPM on 28 February 2022, in the same manner as the patient described above. She had postoperative nausea, which aggravated on POD#3. Her abdomen X-ray demonstrated mild ileus, which aggravated over time (Fig. 2E, F). Her abdominal CT revealed an incisional hernia on the left trocar site accompanied by small bowel obstruction (Fig. 2H). On POD#6, she underwent incisional hernia repair, and bowel perfusion remained unimpaired. She recovered well and her X-rays showed nonspecific findings (Fig. 2G).
Discussion
We reviewed TSH cases following robot-assisted gynecologic surgery from the literature search to identify relevant factors associated with TSH. We searched PUBMED with the keywords “robot,” “trocar site,” “hernia,” and “complications” and found seven reports on TSH during robotic surgery in the gynecologic field [2–8]. Among the literature, an 8-mm TSH was reported in only four cases, excluding our case (Table 1). In contrast to previous studies, which mainly included Caucasian patients who were relatively obese and elderly, our study had an 8 mm TSH occurrence in younger and leaner women. This study is the first case of robot-assisted gynecologic surgery in which a hernia occurred while the drain was in situ. In laparoscopic surgery, a case of bowel herniation occurring 12–48 h after removing a drain at a 5 mm trocar site has been reported [9]. The authors suggested that drains could have facilitated the herniation because they trap or create a suction effect on the bowel when removed. It is valid to consider inserting the drain through a new site with a minimal incision that tightly fits it.
Previously reported cases and our current case on any size of TSH after robotic gynecologic surgery.
| Reference (n = number of hernia case) | Procedure | Diagnosis | Herniated trocar site and size | Age at operation (years old) | BMIat operation (kg/m2) | Incidence of 8-mm site hernia (in an original article) | Time to herniation diagnosed from operation (days) | Fascia closure | Presentation | Image finding | Management |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Seamon et al., 2008 [case report] [6] (n = 1) | Hysterectomy and bilateral salpingo-oophorectomy, pelvic and aortic lymphadenectomy | Endometrial cancer | Left mid-axillary 8-mm robotic trocar site | 67 | – | – | 4 | 12-mm endoscopic port was used to close the fascial defect; the fascia of all lateral port sites were not closed | Nausea, bilious vomiting, and abdominal distention, Small bowel obstruction | Small bowel herniation and obstruction | Nasogastric tube for decompression, Exploration (bowel reduction and fascia repair) |
| Clark et al., 2013 [original article] [2] (n = 3) | Unilateral salpingo-oophorectomy | Benign | Left upper quadrant, 10-mm port | Median 44.5 | – | 0% (all in 12-mm trocar sites) | 38 | Single stitch of 0-Vicryl at all 12-mm port sites, no fascia closure at 8-mm trocar site | Bulge on postoperative examination | Herniation | Conservative management |
| Pelvic lymphadenectomy (LND) for staging | Malignancy | Umbilical, 10-mm camera port | 21 | Postoperative nausea | Herniation | Conservative management | |||||
| Pelvic LND for staging | Malignancy | Left upper quadrant, 10-mm port | 8 | Acute pain, small bowel obstruction | Small bowel herniation | Emergent laparoscopic reduction of hernia and hernia repair | |||||
| Kilic et al., 2013 [case report] [4] (n = 1) | 4-port robotic hysterectomy and bilateral salpingo-oophorectomy | Benign | 8-mm port site | 53 | 30 | – | 3 | 12-mm port was closed with 2–0 vicryl, the fasciae of the 8 and 5-mm port sites were not closed | Right lower quadrant pain and dark coffee-colored vomitus. Tender nodule in the right lower quadrant | Small bowel obstruction at the right anterior axillary 8-mm port site | Emergent laparoscopic bowel reduction and hernia repair |
| Boone et al., 2013 [original article] [3] (n = 0) | In suspected gynecologic patients (Robot-assisted total laparoscopic hysterectomy (TLH) ± unilateral or bilateral salpingo ± oophorectomy (USO/BSO) ± LND ± omentectomy (OMX)) | Malignancy + benign | None | Mean 55.6 | Mean 33.6 | 0% (no hernia case) | – | Fascial closure was not routinely performed except after specimen removal through the port site | – | – | – |
| Schiavone et al., 2016 [original article]$ [5] Cybulska et al., 2017 [original article]& [7] (n = 11) | Staging surgery (robotic vs. laparotomy)$ Staging surgery (robotic vs. standard laparoscopic surgery)& | Endometrial cancer | Ten patients in midline defects (12-mm), one patient at a lateral defect of a prior inferior epigastric port site (8-mm). | Median 66 | Median 38.8 | 0.18% (1/567) | 18.5 months for the umbilical hernias, 7 months for the supraumbilical hernias, and 8 months for the lateral defect | No 8 mm-site closure | – | – | Elective laparoscopic surgical repair in four patients |
| Micelli et al., 2019 [case report] [8] (n = 1) | Colposacropexy and adnexectomy | Prolapse | 8-mm left lateral trocar site | 74 | 21 | – | 3 | No 8 mm-site closure | Generalized malaise and acute abdominal pain in the lower left quadrant | A small bowel dilatation with a transition point along the left lateral 8 mm trocar site | Laparotomy and small bowel resection due to incarcerated ischemic small bowel loop, closure of wall defect |
| The present case (n = 2) | 3PRM | Myoma | Left mid-axillary line 8-mm robotic trocar site | Mean 44.5 | Mean 22.54 | – | 3.5 | Single-port site closure. No 8 mm-site closure | Nausea, vomiting, and abdominal distention | Small bowel herniation and obstruction | L-tube for decompression, Exploration (Bowel reduction and fascia repair) |
POD: postoperative day.
BMI: body mass index.
$, &: In both papers, the same group performed the studies. They compared the surgical outcomes in robotic surgery vs. laparotomy, and robotic surgery vs. laparoscopy in same robot patients.
In the past, efforts have been made to identify the risk factors associated with TSH, but no definite factor has been identified. Some suggested risk factors for TSH sin laparoscopic surgeries include obesity, lengthy operation time, trocar type, opened fascial defect, stretching the port site, and trocar size [9, 10]. Unlike laparoscopy, the difference in robotic surgery is that the robot arm is directly connected to the port site for manipulation. Robotic arms inflict great force on the abdominal wall [6]. Also, robotic arms have a higher range of motion with greater rotating capacity compared with the hand motion of conventional laparoscopy. Thus, robotic surgery has a high chance of expanding the fascia defect [4].
Whether the fascia of the 8-mm ports should be routinely closed after robotic surgery remains controversial. Diez-Barroso et al. hypothesized the sliding effect of the rectus abdominis muscles as one of the plausible explanations for TSH occurrence at the 8-mm port site near the iliac crest. When deflated, the areas where the external oblique, the internal oblique, and the transversus abdominis muscles overlap can fill the trocar holes by sliding over each other in a different direction. However, the point of insertion on the aponeuroses and tendons of the muscle does not have this effect, causing hernia to occur more frequently [11]. The robotic 8 mm trocar insertion point is vulnerable site where aponeurosis or tendon of abdominal wall muscles is located (Fig. 1B). Since the protective effect of the muscle cannot be expected, there is a high possibility of TSH occurring at any time until the defect is sealed.
One of the easiest ways to prevent TSH is to adopt fascia closure in 8-mm-port. Alternative methods to fascia closure, such as applying Surgicel® plugs (Ethicon Endo-Surgery, Cincinnati, OH, USA), have also been introduced in previous literature [9]. Another critical factor to consider is correctly setting remote center when initially setting the robot and during the surgery to avoid excessive force. When setting the robot, trocar insertion should be done vertically. After docking the robot, the position of remote center should be double-checked just before the instrument insertion. Finally, the position of the remote center should be checked frequently during the surgery, especially when there have been changes in abdominal pressure.
In conclusion, since it is difficult to predict 8-mm TSH, it is essential to set an established protocol for minimizing such cases. Early diagnosis of TSH is key to minimizing patient harm; physicians should suspect it when there are abnormal symptoms after surgery. It may be beneficial to reconsider fascial closure of lateral trocar sites after robotic surgery.
Author contributions
Yeon Hee Hong (Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing—original draft, Writing—review & editing), Haerin Paik (Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing—original draft, Writing—review & editing), Seul Ki Kim (Formal analysis, Investigation, Writing—review & editing), Jung Ryeol Lee (Conceptualization, Investigation, Project administration, Supervision, Writing—review & editing), Chang Suk Suh (Investigation, Supervision, Writing—review & editing).
Conflict of interest statement
None declared.
Funding
None declared.
Ethics approval
This report was approved by the Institutional Review Board (IRB) at our institution (IRB number B-2202-737-701).
References
Author notes
Yeon Hee Hong and Haerin Paik contributed equally to this work.

{kind=link}
{kind=link}