





Abstract
Duplication of the vas deferens is a rare congenital anomaly, with an incidence of ~0.05% in the general population. It is typically discovered incidentally during surgeries involving the spermatic cord, such as inguinal hernia repair. This case report presents a 33-year-old male who underwent left inguinal hernioplasty, during which duplication of the vas deferens was incidentally identified. The patient had presented with left-sided inguinal swelling, painful testis, and a small left testis. Preoperative ultrasound suggested an inguinal hernia, but the vas deferens anomaly was only detected intraoperatively. The patient successfully underwent hernioplasty without postoperative complications. This case emphasizes the importance of recognizing rare anatomical variations like vas deferens duplication to prevent surgical complications.
Introduction
Duplication of the vas deferens is a rare congenital anomaly, affecting ~0.05% of the general population [1].This anomaly is characterized by the presence of two distinct vasa differentia within one spermatic cord. Embryologically, it may result from duplication of the mesonephric duct system. It is typically discovered incidentally during surgeries involving the spermatic cord, such as inguinal hernia repair, varicocelectomy, vasectomy, or orchiopexy [2]. Recognition of this anomaly is crucial to avoid iatrogenic injury, obstruction, or spermatic granuloma, and to prevent vasectomy failure [3]. Doppler ultrasonography can be used to confirm the absence of waveforms in both vas deferens, distinguishing them from adjacent vessels [4]. Due to its rarity, this condition may be underreported or frequently unrecognized.
Herein, we present the case of a 32-year-old male diagnosed with left inguinal hernia and was found to have duplicated vas deferens. This case report has been reported in line with SCARE 2023 guideline [5].
Case report
A 33-year-old male with no known comorbidities presented to our surgical outdoor patient department with chief complaints of left-sided inguinal swelling for 3 months, left-sided painful testis and small left testis. He was well three months back when he developed swelling on the left inguinal side, which was painless, which used to aggravate coughing and walking and used to decrease when doing rest. Associated with it, he also had a painful testis and a small left testis. He denied any urinary or abdominal symptoms. Other past medical, surgical and family histories were not significant.
On examination, the patient was conscious, oriented to time, place, and person, and all the vitals were stable. Examination of the left inguinal region revealed swelling on the left inguinal region, which was present in standing and supine position. The swelling was reducible with a negative transillumination test. A cough impulse was present on the left swelling side. The swelling was extended up to the scrotal base. The patient had no other history of swelling or vascular engorgement.
Upon laboratory investigations, blood parameters including white blood cell counts, hemoglobin, packed cell volume and mean corpuscular volume were normal. Further biochemical investigation of sodium, potassium, serum urea, and serum creatinine were normal. Further serological tests were not significant. Ultrasound of bilateral inguinal scrotal region was performed and suggested a left-sided inguinal hernia with protrusion of omental fat and bowel loop through a defect of size 1.2 cm into the left inguinal canal, which was partially reducible, with a left-sided small testis and right-sided minimal hydrocele.
The patient underwent open inguinal hernioplasty via sub arachnoid block anaesthesia. A linear incision was given during the surgery, and the dissection of the left inguinal region and indirect inguinal sac with omentum was identified. Further exploration of the inguinal sac and adjacent cord structure identified two separate vas deferens draining to the left testis, which were positioned anteromedially to the hernial sac (Figs 1 and 2) Both the anomalous vas defentia were draining to the left testis, which was further confirmed by palpation. Further examination of the left scrotum revealed small-sized testis and ectopic left-sided testis. Caudally, both vasa deferentia were communicating separately with the tail of the epididymis. After that, hemostasis was maintained, and the dressing was done. The patient tolerated the procedure.
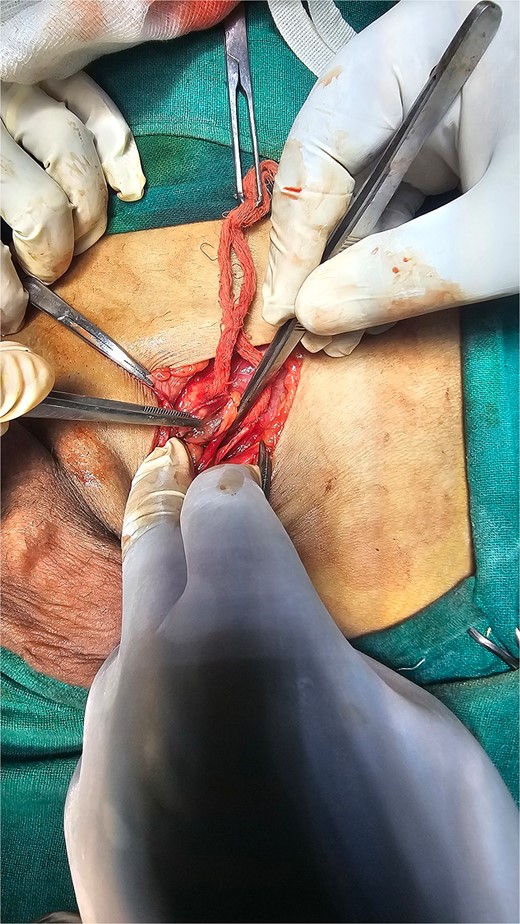
Duplicated vas deferens emerging from a single testicle during spermatic cord dissection during operative procedure.

Duplication of vas deferens.
There were no postoperative complications such as recurrence of the hernia, hematoma, scrotal oedema, and urinary retention. The patient was discharged the day after surgery with no postoperative complications. Follow-up was done, and he did not report any fertility issues or masses in the region of the surgery.
Discussion
The vas deferens is a complex muscular tube and innervated by hypogastric nerve, which releases neurotransmitters like noradrenaline and ATP, affecting smooth muscle contraction and epithelial ion transport [6]. Anatomic variations of the vas deferens include absence, duplication, ectopia, hypoplasia, and diverticulum, with true duplication the rarest congenital anomaly. These anomalies can be classified into several categories, including bilateral agenesis, unilateral agenesis, and duplication [7]. Vas deferens abnormalities can result from various causes and impact fertility. Unilateral duplication of the vas deferens is a rare congenital anomaly [3]. Duplication of the vas deferens is a rare congenital anomaly often discovered incidentally during surgeries involving the spermatic cord [2]. The estimated incidence is ~0.05% of the general population, but it may be underreported due to lack of recognition [8]. This condition can occur unilaterally or bilaterally, with the duplicated vas deferens typically communicating separately with the epididymis and fusing at the deep inguinal ring [9]. This condition is typically discovered incidentally during inguinal hernia repair, vasectomy, or other urological procedures [7].
While preoperative diagnosis is practically impossible, intraoperative recognition is crucial to avoid complications like failed vasectomy or iatrogenic injury [10]. Doppler ultrasonography can help differentiate duplicated vasa deferens from adjacent vessels [3]. In this, preoperative ultrasonography of bilateral inguinal scrotal region was sent, and the result was, left sided inguinal hernia with left sided testis only. Recognition of this anomaly is crucial to avoid surgical complications, including unsuccessful vasectomy or iatrogenic injury to the vas deferens [11]. Duplication of vas deferens may be associated with other non-testicular genitourinary anomalies, warranting careful examination [12]. Timely intraoperative diagnosis of duplication anomaly prevented our case from surgical complication and follow up was carried out to check for fertility and he did not report any fertility issues or masses in the region of the surgery. Duplication of vas deferens can occur unilaterally or bilaterally and may be associated with other conditions such as cryptorchidism or ectopic testis [13]. Our case had unilateral duplication of vas deferens as an anomaly and ectopic testis along with small testis. Because the number of hernia repair procedures performed each year is considerable worldwide, surgeons need to be aware of this anatomic anomaly to lower the risk of damage and unfavorable post-surgical outcomes [14].
Conclusion
Duplication of the vas deferens is a rare congenital anomaly often discovered incidentally during surgical procedures such as inguinal hernia repair. Intraoperative recognition is essential to avoid complications like iatrogenic injury or failed vasectomy. This case highlights the importance of awareness among surgeons of such anomalies to prevent surgical complications.
Author contributions
Bibek Shrestha (Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Original writing, Review, Editing, and Visualization), Krishna Yadav (Resources, Supervision, Validation, Conceptualization, Investigations, and Data curation), Sachet Subedi (Supervision, Validation, and Investigations), Grishma Kandel (Supervision, Validation, and Investigations), Pratibha Yadav (Supervision, validation, and investigations).
Conflict of interest statement
None declared.
Funding
None declared.
Provenance and peer review
Not commissioned, externally peer reviewed.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Guarantor
Dr. Krishna Yadav.

{kind=link}
{kind=link}