





Abstract
Giant thrombotic aneurysms of the anterior cerebral artery (ACA) are rare and pose significant challenges due to their variable clinical presentations. While complications following surgical interventions for these aneurysms are known, they have not been fully characterized. We present a novel case of postoperative infarction in the recurrent artery of Heubner (RAH) following resection of a thrombotic giant aneurysm in the ACA. A 53-year-old man with no prior systemic illnesses presented with progressive weakness in his left hand and foot, along with slurred speech. Imaging studies revealed a giant thrombotic aneurysm in the proximal A2 segment of the right ACA, which was completely occluded. Additionally, a chronic infarction was identified in the territory of the right ACA. The patient underwent successful surgical resection of the aneurysm. However, he subsequently developed an infarction in the RAH territory, a complication rarely reported in the literature. This case highlights the importance of comprehensive preoperative evaluation and underscores the need to anticipate and manage potential complications following surgery.
Introduction
Giant aneurysms, accounting for only 3%–5% of all intracranial aneurysms, pose a significant challenge due to their heterogeneity and complex vascular anatomy [1–3]. Defined as exceeding 2.5 cm in diameter by Sekhar et al. [4], these aneurysms are notable for their frequent development of intraluminal thrombosis, occurring in 10%–30% of cases [5]. Despite advancements in diagnostic imaging and neurosurgical techniques, managing giant aneurysms remains complex, requiring a highly individualized, multidisciplinary approach [6, 7].
Thrombotic giant aneurysms present serious complications due to their size and the potential for thrombosis [8–10]. The recurrent artery of Heubner (RAH) supplies vital structures like the head of the caudate nucleus and the internal capsule. It is a potential site for complications following surgical clipping of aneurysms [11, 12]. A study involving 1043 patients who underwent surgery for intracranial aneurysms reported that 4.4% of the patients experienced infarctions in the area of the perforating arteries post-surgery [13]. Despite the higher risk of postoperative infarction associated with giant thrombotic intracranial aneurysms, there have been no reported cases of RAH infarction following surgery for such aneurysms. Here, we present a rare case of a 53-year-old male with a giant thrombotic aneurysm in the right anterior cerebral artery (ACA) who developed an infarction in the RAH territory after surgical resection of the aneurysm.
Case report
A 53-year-old man with no prior history of systemic illness reported experiencing intermittent weakness in his left hand for several years. This weakness progressed to his left foot over the past 6 months, and he developed slurred speech within the last month. These symptoms prompted him to seek emergency care.
Blood tests revealed elevated glucose (152 mg/dl) and alanine transaminase (ALT) levels (116 U/L), while other parameters were normal. Brain magnetic resonance imaging (MRI) showed a giant thrombotic aneurysm in the proximal A2 segment of the right ACA near the anterior communicating artery (A-com). The aneurysm was completely occluded, and a chronic infarction was present in the territory of the right ACA (Fig. 1).
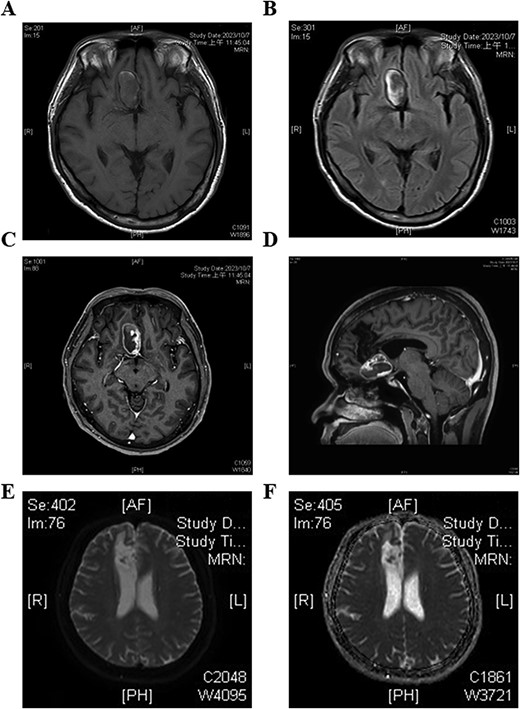
Preoperative brain magnetic resonance imaging (MRI) of the patient reveals a giant aneurysm in the right frontal area. (A) T1-weighted image shows the mass as hypointense. (B) T2-FLAIR image shows hypointensity in the center with peripheral hyperintensity. (C, D) Contrast-enhanced T1 images demonstrate peripheral contrast stasis around the mass, with no enhancement observed in the distal right anterior cerebral artery (ACA). (E, F) Diffusion-weighted image (DWI) and apparent diffusion coefficient (ADC) images show infarction in the areas supplied by the right distal ACA.
After expert consultation, it was decided that this aneurysm would be treated via surgical resection. The craniotomy was performed using the standard right pterional approach. During dissection, the first temporal clip was applied to the right A1 segment of ACA for proximal control. After identifying the origin of the aneurysm and the anterior communicating artery (Fig. 2A), a permanent clip was placed on the proximal A2 segment (Fig. 2C). The temporal clip was subsequently removed, with a control time of 4 minutes and 30 s. Another permanent clip was applied to the right distal A2 segment to avoid backflow to the aneurysm. Upon incision of the aneurysm, it was confirmed to be completely thrombosed with the presence of old blood and thrombus (Fig. 2B). Despite the complexity of the giant aneurysm and the reduced vessel size due to chronic occlusion, every effort was made to preserve all visible branches to the best of our ability. The aneurysm, measuring ~4 cm, was then excised (Fig. 2D). After routine hemostasis, the dura, skull, and scalp were closed in layers.
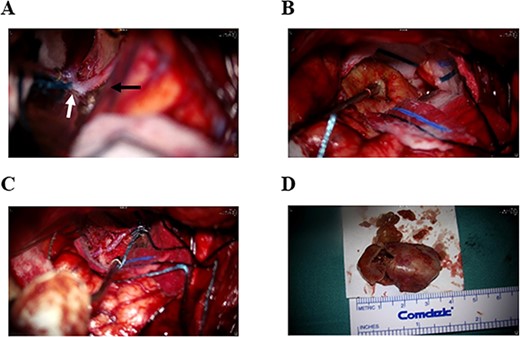
Intra-operative images. (A) The right A1 segment (black arrow) and anterior communicating artery (white arrow) are patent. (B) The giant aneurysm is completely occluded, showing no arterial flow. (C) The aneurysm clip is applied to the right A2 segment of the ACA before resection of the aneurysm. (D) The fully resected giant aneurysm measures ~4 cm in size.
Four hours postoperatively, the patient experienced a generalized tonic–clonic seizure, requiring emergency intubation and sedation. Emergent post-operative brain computed tomography angiography confirmed that the right A1 segment was patent with no signs of intracerebral hemorrhage (ICH) or extradural hematoma (Fig. 3). Brain MRI, however, revealed a new infarction in the RAH territory (Fig. 4). To enhance perfusion, we maintained the blood pressure with a mean arterial pressure >65 mmHg and provided adequate hydration using normal saline. Antiepileptic medication was administered with levetiracetam 500 mg every 12 hours. Antiplatelet or anticoagulant medications were not given.
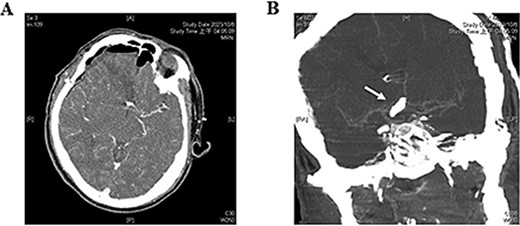
Postoperative brain computed tomography angiography. (A) No immediate signs of intracerebral hemorrhage or epidural hematoma are observed. (B) The patency of the A1 segment (white arrow) of the ACA is confirmed.
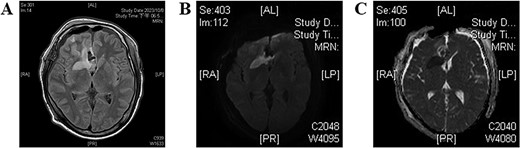
Postoperative brain MRI. (A) T2-weighted image shows a hyperintense area, indicating acute infarction of the recurrent artery of Heubner. (B, C) Findings are consistent with the abnormalities observed on the DWI and ADC images, respectively.
On postoperative Day 5, after tapering sedation, the patient returned to a fully clear state and was successfully weaned off the ventilator. A detailed neurological examination at this time revealed a Glasgow Coma Scale score of E4V5M6, with left-sided limb strength grade 2. Subsequent electroencephalography showed no epileptiform discharges. During the hospital stay, with adequate rehabilitation, the strength in the left-sided limbs gradually improved to grade 3. By the time of discharge on the 14th postoperative day, the patient was able to walk independently. At 3- and 6-month post-surgery, except for slightly reduced strength in his left hand (grade 4), all other muscle strength had returned to the pre-operative status. At 6 months post-surgery, follow-up angiography showed no recurrence of the aneurysm, and a functional assessment indicated a Modified Rankin Scale of 1. The Mini-Mental State Examination score was 30, with no deficits in cognitive or speech function. The patient has since been followed up in the outpatient clinic for a year, with no subsequent complications or recurrence.
Discussion
Nature history of unruptured/thrombotic giant aneurysm
Giant aneurysms, representing only 3%–5% of all intracranial aneurysms, exhibit a significant female predominance with a sex range from 2:1 to 3:1 [3, 14, 15]. Spontaneous thrombosis within these large aneurysms occurs in 13% to 60% of cases [5, 16–18]. Approximately 70% of patients with giant aneurysms experience symptoms due to mass effects, such as headaches and neurological deficits [19, 20]. Notably, ~25% of these patients first present with a subarachnoid hemorrhage or ICH [15, 21]. Seizures are another presenting symptom, occurring in up to 5% of cases [19].
The PHASES study confirms that larger aneurysms carry a higher risk of rupture [22]. However, the presence of partial or complete thrombosis within giant aneurysms, traditionally considered protective against bleeding, presents a complex picture. While such thrombosis may indeed lower the risk of bleeding, it also increases the risk of thromboembolic events, creating a different set of complications.
Management of giant thrombotic aneurysm
There are no definite guidelines for treating giant thrombotic aneurysms. The primary aim of any intervention is to reduce blood flow into the aneurysm sac. This stabilizes its structure, prevents rupture, and alleviates symptoms caused by its mass effect. Available treatment options fall into two broad categories: microsurgical techniques like clip reconstruction, and endovascular strategies such as coil embolization and intracranial stents [4, 23]. A thorough evaluation of both microsurgical and endovascular approaches is crucial for making informed treatment decisions, considering the potential complications associated with each method. Transarterial embolization remains an alternative approach.
Postoperative stroke after surgical resection of giant aneurysm
Arun Balaji et al. [24] documented that among 52 patients who underwent microsurgery for large and giant intracranial aneurysms, there were a total of 6 complications, accounting for 11.5% of all cases, with no surgical mortality. However, this study did not report any cases of postoperative infarction. Qazi et al. [25] also conducted a postoperative analysis of patients with very large and giant aneurysms. In the unruptured group of 52 patients, 4 (7.69%) experienced postoperative strokes. Li et al. [26] documented a higher rate of postoperative complications, with 6 out of 12 surgical patients experiencing postoperative complications, including 4 cases of postoperative stroke. Although the risk of thromboembolism is lower after aneurysm clipping compared to aneurysm embolization, branch artery occlusion can occur during thrombectomy and clipping reconstruction. This may result from embolic displacement of the thrombus during or after the thrombectomy procedure.
Causes of RAH infarction
Preservation of the RAH is crucial due to its significant role in supplying blood to critical areas of the basal ganglia, particularly the caudate nucleus and the anterior limb of the internal capsule. During the resection of giant aneurysms in the ACA, meticulous attention to the RAH is essential to minimize postoperative neurological deficits. To our knowledge, this report is the first to describe postoperative infarction of the RAH following surgery for a thrombotic giant aneurysm in the A2 segment. The causes of postoperative RAH infarction are multifactorial, as evidenced by previous studies [11, 27]. In this case, we considered three potential mechanisms, given the patient’s lack of reported systemic disease.
The first mechanism involves direct injury to the RAH during surgical resection. This could be caused by inadvertent occlusion from blockage or constriction of the artery, possibly due to intraoperative manipulation, compression, or tension placed on the vessel. The second potential cause is a thromboembolic event occurring during surgery. This might arise from intraoperative embolization of a clot, clot formation within the surgical field, or perioperative events such as hypoxia. The third theory centers on prolonged ischemia caused by temporary clipping of the A1 segment during dissection. Extended use of temporary clips may restrict blood flow to the RAH, leading to ischemic injury.
Learning from this case
While MRI confirmed complete thrombosis of the aneurysm and occlusion of the distal segment of the ACA, cerebral angiography remained crucial for delineating any critical small perforating branches and collateral circulation. The ACA supplies vital deep brain structures through a network of these small perforators. Missing these on preoperative imaging can lead to inadvertent vessel compromise and subsequent neurological deficits. Additionally, the ACA can develop collateral pathways in response to occlusion, which is essential for maintaining cerebral perfusion when the primary arterial route is blocked.
Limitations
The absence of preoperative digital subtraction angiography (DSA) limited our ability to assess the patient’s vascular anatomy. DSA is invaluable in preoperative planning as it allows for the detailed identification of critical vascular structures, which are crucial for guiding surgical strategy [28]. DSA offers superior visualization of the cerebral vasculature. Capturing images before and after contrast injection allows subtraction of non-vascular structures, resulting in clearer views of blood flow dynamics. Preoperative DSA could have provided invaluable insights into the vascular network, potentially affecting our surgical approach by revealing a roadmap of small perforators and collateral vessels. The omission of DSA limited our ability to anticipate and protect these vessels during surgery, which could have significantly impacted postoperative recovery and patient outcomes.
Conclusion
This case report, the first to describe RAH infarction following resection of a giant thrombotic A2 segment aneurysm, underscores the critical importance of comprehensive preoperative evaluation. It also sheds light on the inherent challenges associated with managing giant thrombotic aneurysms. Furthermore, it highlights the necessity of anticipating and planning for potential postoperative complications.
Acknowledgements
None.
Author contributions
K.-H.F. studied concepts, statistical analysis, manuscript preparation, manuscript editing. P.-Y.Ch. studied concepts, data acquisition, data analysis, statistical analysis, manuscript review. J.-L.Y. studied concepts, study design, clinical studies, manuscript preparation, manuscript editing, manuscript review. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declare that they have no competing interests.
Funding
None declared.
Data availability
All of the data supporting underlying findings are included in the manuscript and its supplemental files.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}