





Abstract
The authors presented a case of duodenal obstruction in a 61-year-old man, resulting from an annular pancreas diagnosed on imaging (computed tomography, magnetic resonance cholangiopancreatography, and endoscopic ultrasound). The patient underwent a diagnostic laparoscopy. Intraoperatively, given a straightforward appearance and anatomy of the annular pancreas overlying the second part of the duodenum, and due to extensive adhesions in the abdomen, a primary division of the annular pancreas was performed, instead of a bypass procedure such as gastrojejunostomy. He had some residual symptoms 1 week postoperatively which was treated with duodenal dilatation endoscopically. On review and follow-up at 1 year, he has remained well with resolution of symptoms, supported by radiological improvement on a computed tomography performed at 4 months post-operatively. We believe this approach has resulted in less morbidity and a shorter period of recovery as compared to a bypass procedure and represents a reasonable therapeutic option for annular pancreas.
Introduction
Annular pancreas in adults is extremely rare. However, it can result in symptoms of duodenal obstruction and the existing literatures suggest surgical treatment by a bypass procedure such as gastrojejunostomy. Here, we illustrate the utility of laparoscopic primary division of an annular pancreas which has not been reported previously.
Case
A 61-year-old man presented with 4 days of epigastric discomfort, reflux, belching, and constipation (passing small amounts of flatus however with bowels not opened for 10 days). He had an open Nissen fundoplication completed for reflux symptoms 30 years ago. He had longstanding postprandial fullness and abdominal discomfort, and this was attributed to recurrent gastro-oesophageal reflux disease; however, he was not medicated for this. He was an ex-smoker and consumed alcohol on a regular basis. Abdominal examination revealed a long midline laparotomy with multiple incisional herniae. On palpation, the abdomen was soft but tenderness was elicited in the upper abdomen, however without peritonism.
The patient was admitted for further work-up. A computed tomography (CT) scan revealed a duodenal outlet obstruction with a transition point at the level of the pancreatic head with periduodenal fat stranding and duodenal wall thickening, with the impression of enhancing pancreatic tissue lateral to the duodenum at this site (Fig. 1). Magnetic resonance cholangiopancreatography (MRCP) suggested an abrupt transition in the caliber of the second part of the duodenum by an obstructive periampullary lesion, through which a dilated extrahepatic bile duct (9 mm) passed through (Fig. 1). The pancreatic duct size was normal with no surrounding lymph node enlargement or vascular encasement by the pancreatic parenchyma. His liver enzymes and serum tumor markers (carbohydrate antigen 19–9 (CA19–9), carcinoembryonic antigen, and alpha-feto protein) were unremarkable. His serum lipase level was 171 U/l. An endoscopic ultrasound (EUS) of the upper gastrointestinal tract was performed to assess the obstructive periampullary lesion (Supplementary Video 1).
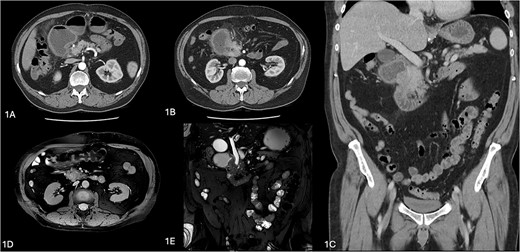
Radiological images of annular pancreas. (A–C) Computerized tomography images showing duodenal obstruction with a transition point at level of pancreatic head with periduodenal fat stranding and duodenal wall thickening, with impression of enhancing pancreatic tissue lateral to duodenum at this site. (C, D) Magnetic resonance cholngiopancreatography images showing an abrupt transition in the caliber of the second part of the duodenum by an obstructive periampullary lesion, the annular pancreas.
An annular pancreas was suggested by the CT and MRCP, and the diagnosis of a complete annular pancreas was confirmed on EUS. Consideration was given for malignancy of the pancreatic head, but this was ruled out with normal tumor markers and biochemical markers and EUS findings (no discrete pancreatic mass or lesion otherwise).
Given his presentation with a duodenal outlet obstruction, a bypass procedure (gastrojejunostomy) was initially recommended. The abdomen was explored via laparoscopy with extensive division of anterior abdominal omental adhesions. A grossly dilated stomach and the first part of duodenum were visualized in the right upper quadrant of the abdomen. Mobilization of the hepatic flexure exposed the paracolic gutter revealing the annular pancreas overlying the second part of the duodenum.
Intraoperatively, given a straightforward appearance and anatomy of the annular pancreas overlying the second part of duodenum, coupled with extensive adhesions from the patient’s previous open abdominal surgery, a decision was made to perform primary division of the annular pancreas to relieve the duodenal obstruction. A plane was developed between the posterior surface of the annular pancreas overlying the anterior portion of the second part of the duodenum (Fig. 2, Supplementary Video 2), allowing placement of a laparoscopic stapler (Covidien articulating Endo GIA™ vascular/medium tri-staple 45 mm (gold)) in this space to transect the annular pancreas (Figs 3 and 4, Supplementary Video 2). A laparoscopic cholecystectomy was also completed as the patient had extensive cholelithiasis, and an intraoperative cholangiogram demonstrated pancreaticobiliary malunion with the bile duct entering the main pancreatic duct proximal to the ampulla (Fig. 5, Supplementary Video 2), which is an abnormality known to be associated with annular pancreas [1]. A 10-French Jackson-Pratt drain tube was placed in the right upper quadrant of the abdomen and over the site of the annular pancreas division. An intraperitoneal mesh was placed laparoscopically to repair his multiple incisional hernia and secured with transfascial sutures and AbsorbaTack™.
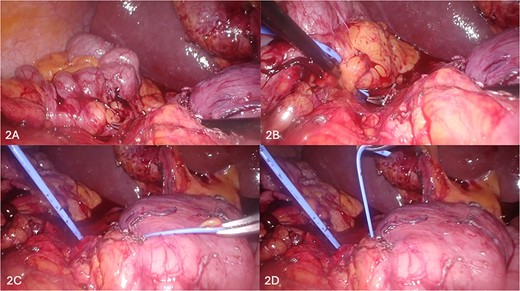
(A–D) Sequential depiction of the plane between annular pancreas and duodenum being defined using Maryland grasper (A, B) and silicone vessiloop (B–D).
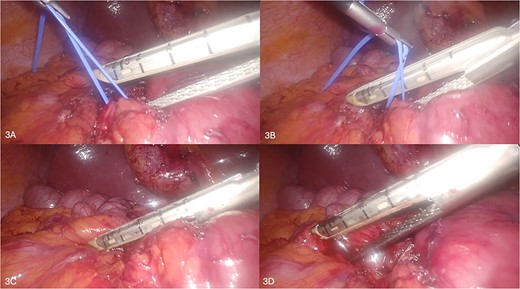
(A–D) Sequential depiction of the division of annular pancreas using laparoscopic stapler device.
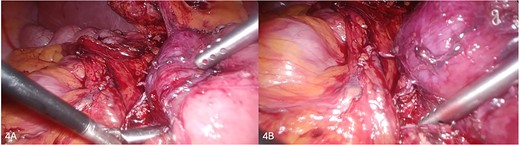
(A, B) Successfully transected annular pancreas above duodenum.

Intraoperative cholangiogram showing pancreaticobiliary malunion with the bile duct entering the main pancreatic duct proximal to the ampulla.
The patient was able to tolerate a normal diet from the first post-operative day with minimal and reduced epigastric discomfort. Given the division of the pancreas had been performed, a routine drain tube lipase was sent on the third postoperative day, which returned a result of 708 U/l and indicated a small pancreatic leak. As the patient remained clinically well, the pancreatic leak was managed conservatively with the drain tube left in situ, and the patient was discharged home with a hospital home-visiting service for drain tube management and for outpatient follow-up in 2 weeks’ time.
The patient represented on the eighth postoperative day with recurrent reflux and belching symptoms. A repeat CT and EUS were performed which demonstrated a 1–2-cm collection adjacent to the second part of duodenum where the annular pancreas had been divided. This was aspirated by EUS and revealed a lipase of 88 931 U/l, consistent with a small contained pancreatic leak. At the same procedure, he underwent duodenal dilatation with a CRE™ balloon dilator placed under fluoroscopic guidance to dilate the duodenal lumen to 20 mm diameter. This has since resolved his symptoms and he has remained well. A repeat CT at 4 months showed improvement of the long-standing gastric distension and first part of duodenum at the previous transition point and resolution of the periduodenal fat stranding and duodenal wall thickening (Fig. 6).
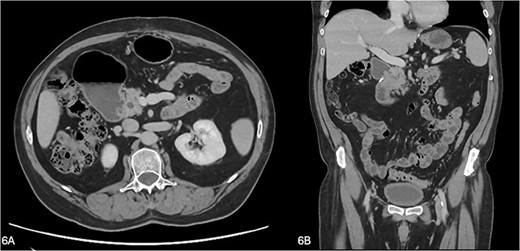
(A, B) A repeat CT at 4 months showing improvement of the gastric and duodenal distension proximal to the previous transition point and resolution of the periduodenal fat stranding and duodenal wall thickening.
Discussion
Annular pancreas is a rare congenital anomaly resulting from a complete or partial ring of pancreatic tissue surrounding the second part of duodenum. Many cases of annular pancreas remain asymptomatic for life, but a small proportion of adults present between the third and sixth decade of life with abdominal pain, duodenal obstruction, or pancreatitis. The annular pancreatic duct can drain to the main pancreatic duct but can communicate with the intrapancreatic common bile duct, the duct of Wirsung, or the duct of Santorini. According to Yogi et al., the two most common types are the annular pancreatic duct communicating with the duct of Wirsung (Type 1) and the duodenum being encircled by the main pancreatic duct [1]. Previous literature (the majority as case reports) describes the treatment of those with symptomatic annular pancreas by performing duodenal bypass procedures such as duodenoduodenostomy, duodenojejunostomy, or gastrojejunostomy [2, 3].
In the above-presented case, given the extensive adhesions, the concurrent incisional hernias, and the favorable pancreatic anatomy, we decided on the laparoscopic division of the annular pancreas rather than enteric bypass, accepting the risk of incomplete relief of obstruction which was further treated with a duodenal balloon dilatation via endoscopy. We believe that the procedure has resulted in less morbidity and a shorter period of recovery as compared to a bypass procedure and represents a reasonable therapeutic approach to the annular pancreas.
Conflict of interest statement
The authors disclose no conflicts. The authors confirm that the material has not been published previously and is not submitted for publication elsewhere.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}