





Abstract
Coronal-plane intra-articular fractures of the femoral condyle (Hoffa fractures) are rare, and difficult to diagnose and treat. They mostly result as a consequence of high-energy trauma and are combined with concomitant fractures (patellar, tibia shaft) and/or soft-tissue damage. A plain X-ray can miss the diagnosis initially and therefore computerized tomography scan is recommended, which can also help in the preoperative planning. The vast majority of these fractures are unicondylar (mostly lateral condyle fractured). The approach for their treatment can be anterior or posterior. In cases of fracture comminution, much more mutilant approaches with osteotomy have been described. A combined two-stage approach can be used to obtain anatomical reduction and fixation of all the fragments. We present a case of a 46-year-old male patient with comminuted lateral Hoffa fracture treated with a combined approach (extended posterior approach to the proximal tibia and lateral parapatellar) in a time interval of one month.
Introduction
Hoffa fracture is defined as a coronal-plane intra-articular fracture of the femoral condyle (medial, lateral, or bicondylar). The fracture might be isolated or combined with the femoral shaft and/or patellar fracture [1]. In general, they are the rarest type that occurs in around 10% of all patients with distal femur fractures [2]. However, unicondylar Hoffa fractures occur in <1% (0.65%) of all femoral fractures [3]. The most common mechanism of injury described is high-energy trauma (falls and traffic accidents), but low-energy trauma in children and osteoporotic individuals can also cause it. The treatment of Hoffa fractures can be challenging and difficult, thus including conservative (in strict narrow indications) and operative (anatomic reduction, stable fixation of the fragments, and early mobilization) [4]. Surgery is associated with certain need for repeated interventions because of fixation failure and/or loss of reduction [1]. We present a case of a male patient with multifragmentary lateral Hoffa fracture with associated ipsilateral patellar fracture treated with a combined open posterior and anterior approach as a two-stage surgery.
Case report
A 46-year-old male patient presented to the outpatient emergency department because of a left knee injury caused by a fall during recreational sports activity. The main complaints were pain in the left knee accompanied by swelling and limited range of motion.
A plain X-ray of the left knee revealed a single defect of the lateral femoral condyle in the anteroposterior (AP) view. The lateral view showed a free bone fragment with a defect (Fig. 1A and B). Additional diagnostic imaging was performed. A computerized tomography (CT) scan revealed multifragmentary (three fragments) fracture of the lateral femoral condyle accompanied by a fracture of the left patella (Fig. 2). The fracture was classified as 33B3.2 according to the Association for Osteosynthesis–Orthopaedic Trauma Association (AO/OTA), Type II C (according to Letenneur) [2]. It was decided that single-approach surgery (posterior or anterior) would be insufficient for acceptable anatomic reduction and proper fixation of all the fragments because of the fracture complexity. The preoperative plan consisted of a posterior-first approach (extended posterior approach to the proximal tibia) for fixation of the largest (posterior) fragment (Fig. 3) followed by an arthroscopic anterior approach (for anterior fragment fixation). The predetermined time interval between the two procedures was to allow the healing of the joint capsule after the index surgery. Operative fixation of the patellar fracture was not indicated.
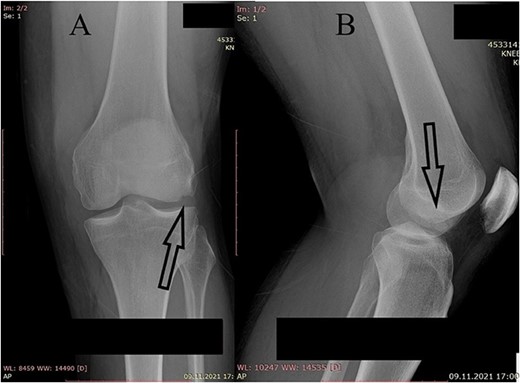
Plain X-ray of the left knee. (A) Anteroposterior view of the left knee with visible bone defect in the lateral femoral condyle (arrow). (B) Lateral view of the left knee with visible free bone fragment (arrow).

CT scan of the left knee (sagittal) with three fragments (arrows) and patellar fracture (arrowhead).

CT scan of the left knee (sagittal) focusing on the largest posterior fragment (arrow).
The patient was positioned in a prone position under general anesthesia. An S-shaped incision was made in the popliteal fossa with proximal extension. The posterior fragment was fixed with two titanium headless compression screws (3.5 mm). The postoperative period was uneventful and the patient was discharged on postoperative Day 6.
One month after index surgery, the patient was readmitted for the second intervention. In spinal anesthesia, the left knee was positioned for routine arthroscopy. During the procedure, it was concluded that the achievement of proper anatomical fragment repositioning and fixation is unobtainable. Therefore, conversion to arthrotomy followed via the lateral parapatellar approach. Fragments were fixed with two titanium headless compression screws (3.5 mm) (Fig. 4). The second postoperative period was uneventful. Early range of motion exercises started on postoperative Day 2. The patient was discharged on postoperative Day 4. The rehabilitation period lasted 4 weeks. Weight-bearing was allowed at Week 8 after surgery.
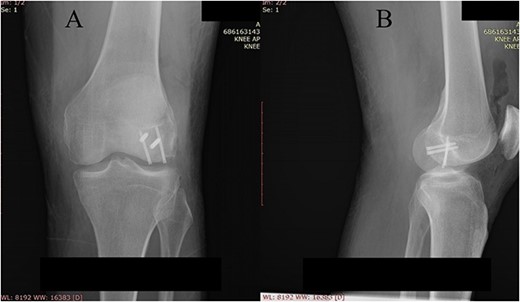
Postoperative plain X-ray of the left knee. (A) Anteroposterior view. (B) Lateral view.
Two years following the injury, the patient had a complete and painless range of motion in the left knee (Fig. 5).

The patient’s range of motion (5 months after surgery).
Discussion
Coronal fractures of the femoral condyle were introduced and described initially by Albert Hoffa in 1904 [4]. According to the AO/OTA classification, Hoffa’s fracture is a tangential unicondylar fracture of the distal femoral condyle. Letenneur further classified Hoffa’s fractures into three types (Types I–III). Of them, Type II is subclassified depending on the fracture line position into A–C subtypes [5].
These fractures might be difficult to diagnose (especially non-displaced ones) and are missed in 30% of cases on plain knee radiographs. CT scan is the gold standard for the diagnosis of Hoffa’s fracture and it allows better visualization of the fragments and allows precise classification of the given fracture. Magnetic resonance imaging should be performed when suspicion of a soft-tissue injury of the knee is raised [4].
Indications for conservative treatment of Hoffa’s fracture are narrow and only non-displaced ones can be treated with cylindrical plaster cast immobilization and the knee positioned at 10° of flexion. This treatment might result in fracture displacement with possible consequences such as nonunion, delayed healing, and posttraumatic arthritis [4].
According to Orapiriyakul et al., surgical planning, approach, and the type of fixation depend on several factors such as condylar blood supply, fracture characteristics, size, plane, and comminution. They describe two groups of approaches (anterior and posterior) with the anterior parapatellar approach being the most commonly used [5]. Several types of fixation have been proposed for Hoffa’s fracture. The most common is the fixation with at least two cannulated screws with/without the addition of a posterior anti-gliding plate [6, 7]. In the series of Gavaskar et al. [2], all 18 patients with isolated Hoffa fractures (OTA type 33-B1) were treated with AP and posteroanterior approach with the use of cancellous screws and headless screws, respectively. In the case report of Soni et al. [8], comminuted medial Hoffa fracture and concomitant patellar fracture fragments were reduced and fixed with L-buttress plate and lag screws. Chandrabose et al. proposed a CT morphological classification with four types of Hoffa fractures (A–D), whereas Type B (articular comminution) refers to the fracture of this case report. They recommend the use of two cancellous screws, whereas in cases of severe fracture impaction, bone grafting was added from the ipsilateral proximal tibia [7].
Arastu et al. point out the importance of posterior comminution presence when an approach is planned for Hoffa fractures. As an option for posterolateral corner knee injuries, they recommend the use of Gerdy’s tubercle osteotomy [9]. In their series, Jain et al. treat the patients with Hoffa and concomitant ipsilateral proximal tibia fractures. Regardless of the fracture type, all patients were treated with some of the standard anterior approaches. However, the authors also discuss the use of Gerdy’s tubercle osteotomy approach for comminuted and complex fractures, although they did not use it [10]. In our opinion, Gerdy’s procedure is a more mutilant one when compared with the extended posterior approach to the proximal tibia (used in this case). To our knowledge, this is the first report of comminuted lateral Hoffa fracture treated with a two-stage combined (posterior and anterior) approach because of the complexity of the fracture.
Reported postoperative complications to comprehend knee stiffness, anterior knee pain, screw displacement and/or migration, lateral collateral ligament laxity, and osteoarthritis [2].
For treatment success estimation, radiologic evaluation and the use of the Shatzker and Lambert scoring system for clinical evaluation are described. Manfredini et al. reported excellent scores (no pain, no deformity, or incongruence; loss of flexion < 10°; full extension) in 37.6% of the patients in their series [3]. In the series of Gavaskar et al. (18 patients), they report knee stiffness and pain in one case treated with AP screw fixation. Lateral collateral ligament laxity (5–10°) was seen in two patients and radiological progression of osteoarthritis by one grade (Kellgren–Lawrence Grades II–III) 12 months after surgery in one patient [2]. In this case, the measured score according to Shatzker and Lambert equals “excellent.”
Comminuted lateral Hoffa fractures are rare and represent diagnostic and therapeutic challenges. Precise diagnosis with the use of CT scan and magnetic resonance imaging should lead to proper diagnosis of Hoffa’s fracture and approach planning. Operative treatment with anatomic reduction and fixation, even two-staged, is expected to result in satisfactory early and late postoperative functional restoration for the affected knee.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}