





Abstract
Hepatic artery pseudoaneurysms are a significant health concern, often incidentally discovered during computed tomography (CT) scans, as their exact incidence rate remains unknown. The most common symptoms of a pseudoaneurysm are hematemesis, abdominal pain, anemia and jaundice. A triad of right upper quadrant pain, jaundice and overt upper gastrointestinal bleeding is a classic presentation of the condition, which occurs in only a third of patients with hemobilia. Patients have a high risk of rupture, and an endovascular approach with coil embolization is recommended. A case of a 28-year-old woman with a post-traumatic hepatic pseudoaneurysm is presented in which she was initially misdiagnosed and treated for cholecystitis. After the development of jaundice, hematemesis and melena, a CT angiography confirmed diagnosis. Endovascular embolization was performed successfully, and the patient recovered without complications. This case highlights the importance of prompt diagnosis of hepatic pseudoaneurysms, as a delayed diagnosis can result in significant morbidity and mortality.
INTRODUCTION
Hepatic Artery Aneurysms (HAAs) and Pseudoaneurysms are infrequent pathologies. The exact incidence is unknown, and most HAAs are discovered incidentally during computed tomography (CT) scans [1]. A retrospective review was conducted to determine the incidence of hepatic pseudoaneurysm after liver trauma and concluded that the incidence increases with a higher grade of liver injury, with >17% of grade V injuries going on to develop pseudoaneurysms [2].
Most pseudoaneurysms present differently from true aneurysms due to their symptomatic manifestation. The most common symptoms are hematemesis, abdominal pain, anemia and jaundice. A classic triad of right upper quadrant pain, jaundice and overt upper gastrointestinal bleeding (Quincke’s triad) has been described, but this occurs in only one-third of patients with hemobilia [3].
In both cases, patients have a high risk of rupture, therefore an endovascular approach with coil embolization is recommended for the affected artery regardless of the cause [1]. This article presents a case of a 28-year-old woman with a post-traumatic hepatic pseudoaneurysm who had the classic triad of Quincke’s and an additional cholecystitis that delayed the diagnosis.
CASE PRESENTATION
A 28-year-old female with no medical history was involved in a motorcycle accident and suffered upper blunt abdominal trauma. She received conservative treatment for severe epigastralgia at a private clinic, and although the pain intensity improved, it did not resolve completely. Five days later, she presented to her local hospital with a sudden onset of epigastralgia after eating and intense pain in the right upper quadrant. During an ultrasound at the hospital, an injury to the right hepatic lobe and several gallstones were observed. Because the abdominal pain was attributed to gallstones, she was managed with analgesics and a low-fat diet during the following weeks. Two months later, she developed jaundice along with hematemesis and melena, which had been ongoing for 3 days, and was admitted to the emergency room. She was stabilized with intravenous fluids and a blood transfusion due to hemodynamic instability.
At this point, she was transferred to our facility. Upon admission, the physical exam revealed intense right upper quadrant pain and jaundice. Her hemogram showed significant anemia and neutrophil predominant leukocytosis (5.7 g/dl and 16.21 10^9/L, respectively), as well as thrombocytopenia (112 10^9/L). Her total and direct bilirubin levels were elevated (total bilirubin 6.5 mg/dl, indirect bilirubin 1.10 mg/dl and direct bilirubin 5.4 mg/dl), as were her serum alkaline phosphatase (255 U/L), liver transaminases (AST 323 U/L, ALT 474 U/L) and procalcitonin (1.08 ng/ml). The renal function test, urine routine and electrolytes were within normal limits.
Based on the patient’s history of liver trauma and current clinical presentation, an intrahepatic vascular injury was suspected. A CT angiography was performed and revealed the presence of a saccular hepatic pseudoaneurysm measuring 5.1 × 4.4 mm in the distal-third of the right hepatic artery (Fig. 1A). The CT scan also showed dilation of the intrahepatic bile duct with a dense image inside, which was consistent with bleeding in the biliary tree (Fig. 1B). In addition, the scan showed a gallbladder with thickened walls and radio dense images inside, compatible with the presence of stones (Fig. 1C).
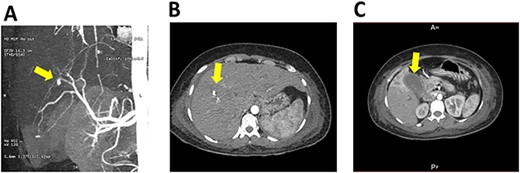
CT scan and angiography of hepatic pseudoaneurysm; (A) saccular hepatic pseudoaneurysm measuring 5.1 × 4.4 mm in the distal-third of the right hepatic artery; (B) the CT scan also showed dilation of the intrahepatic bile duct with a dense image inside, which was consistent with bleeding in the biliary tree; (C) gallbladder with thickened walls and radio dense images inside, compatible with the presence of stones.
To treat the pseudoaneurysm, endovascular embolization was performed without any complications. The procedure was performed through a right femoral artery access using a 5Fr introducer sheath and a 0.035-in guidewire (Terumo Medical Corporation, Japan). An angiography of the celiac trunk was performed using a Cobra catheter and the guidewire and catheter were progressed to the right hepatic artery. An arteriography was performed and the presence of the pseudoaneurysm was identified in the terminal branch of the right hepatic artery along with extravasation of contrast medium in liver segments 5 and 6. The right hepatic artery was embolized with two coils (interlock −35, Boston Scientific Corporation, Marlborough Massachusetts) before its terminal bifurcation. Control angiography showed total exclusion of the pseudoaneurysm with no complications during the procedures.
Following the surgery, the patient’s symptoms, liver dysfunction and hemogram values improved significantly, and the patient was discharged from the hospital after 4 days.
DISCUSSION
We present a case of a hepatic pseudoaneurysm of late presentation after the patient initially exhibited symptoms of cholecystitis. However, after the patient developed signs of upper gastrointestinal bleeding, an Angio CT confirmed the presence of the pseudoaneurysm. The vascular team successfully performed an embolization, and the patient recovered without any complications.
The presentation of a hepatic pseudoaneurysm can range from being an incidental finding in a less acute, symptomatic patient to an acute hemorrhagic shock resulting from a rupture. According to Wagner et al. [2], the median time to identify a hepatic pseudoaneurysm on repeat CT is 6.5 days post-injury. In this case, the patient’s initial clinical findings led the diagnosis to be solely cholecystitis.
Hepatic artery pseudoaneurysm (HAP) is primarily caused by acute or chronic artery injuries from blunt or penetrating trauma or surgical injuries [4, 5]. There have been few reports of other etiologies, such as chronic cholecystitis, which can erode the hepatic artery wall due to inflammation and cause a pseudoaneurysm, but this is less common [6]. In these cases, patients with hepatobiliary diseases, previous authors have considered hemobilia as an important differential diagnosis when gastrointestinal bleeding is observed [7]. Others have also reported bile leak and superimposed infections as important precipitating factors, as they can contribute to injuring the vessel wall and develop a pseudoaneurysm [8].
In this case, the patient seemed to have two precipitating conditions: a hepatic blunt trauma and chronic inflammation of the gallbladder, which may have contributed to the development of the pseudoaneurysm. The hemobilia was the key factor in performing the CT scan, and it should be considered in patients who have suffered recent liver injury with gastrointestinal bleeding.
The diagnosis was complicated by the presence of gallstones and jaundice, which caused confusion and led to a delayed diagnosis. To help avoid such delays, we recommend that healthcare providers investigate HAP in patients with cholecystitis following a blunt abdominal trauma, particularly if their symptoms worsen.
ACKNOWLEDGEMENTS
We acknowledge the Large Language Model ChatGPT (Open AI) for English grammar revision of this manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflicts of interest related to this study.
FUNDING
None.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author, I.S. The data are not publicly available due to their containing information that could compromise the privacy of research participants.

{kind=link}