





Abstract
Femoral hernias accounting for 2–4% of all hernias rarely involve appendicitis, known as De Garengeout hernia, with only a few reported cases. We present a case of a 66-year-old woman with acute right groin pain but no signs of intestinal obstruction. Physical examination revealed a tender, partially reducible mass in the right groin. Computed tomography scan confirmed a femoral hernia containing incarcerated bowel loops, leading to urgent surgical intervention. The McEvedys approach was used for appendicectomy and hernia repair. The patient recovered without complications. Strangulated femoral hernia with the appendix is a rare condition posing diagnostic challenges. Early recognition is crucial to prevent complications like perforation and abscess formation. Cross-sectional imaging aids in diagnosis. Surgical intervention, either open or laparoscopic, is the preferred treatment, based on surgeon expertise and patient-specific factors. Timely diagnosis and prompt surgery minimise complications.
INTRODUCTION
Femoral hernias are relatively uncommon, accounting for ~2–4% of all hernias [1]. While appendix within a femoral hernia, also known as a De Garengeot’s hernia, is a rare occurrence [2], and presents unique diagnostic and management challenges. The combination of strangulated appendix and femoral hernia can lead to potentially life-threatening complications, such as necrosis, perforation and sepsis. We present a case report highlighting a rare occurrence of a strangulated femoral hernia containing the vermiform appendix. Our aim is to emphasise the importance of early recognition, prompt surgical intervention and the potential difficulties encountered in diagnosing and managing this uncommon condition. This case report contributes to the existing literature by expanding our understanding of the clinical presentation, diagnostic modalities and treatment options for appendix within a strangulated femoral hernia. By sharing this case, we aim to improve awareness among clinicians and surgeons about this rare entity, enabling earlier identification and appropriate management of similar cases in the future.
CASE PRESENTATION
We report the case of a 66-year-old female who presented with a short history of sudden onset and worsening pain in the right groin. No symptoms suggestive of bowel obstruction were present. Previous history included an anterior resection, incisional hernia repair and thyroidectomy. On examination, there was a partially reducible, tender and palpable mass. Computed tomography (CT) scan of the abdomen pelvis was performed, which revealed a right femoral hernia and reported as containing incarcerated bowel loops (Fig. 1).
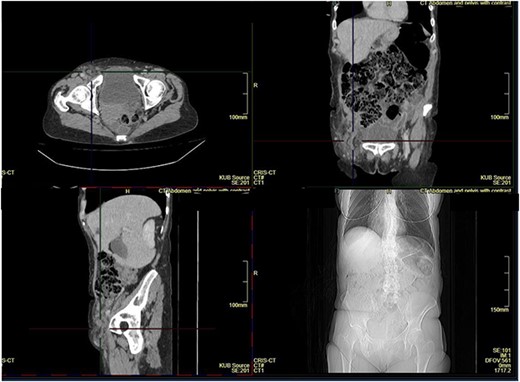
CT scan showing femoral hernia.
The patient underwent surgical intervention. Access was gained to the femoral canal through a high (McEvedy) approach and the hernia sac was identified. The sac was then carefully dissected, content identified and pushed back into the abdominal cavity. The femoral canal is closed using sutures. Abdominal cavity was entered through the McEvedy incision, gangrenous appendix was identified and appendicectomy was performed (Fig. 2). Recovery, postoperatively was uneventful, and the patient was discharged 2 days following surgery.
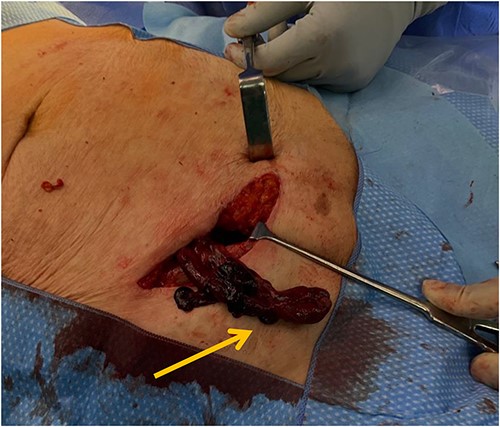
Intraoperative photo showing the femoral hernia containing a gangrenous appendix.
DISCUSSION
The occurrence of an appendix within a strangulated femoral hernia is an extremely rare and challenging clinical scenario. Radiological imaging, including ultrasound and CT scans, can aid in establishing the diagnosis by revealing the presence of an appendix within the femoral hernia sac.
Prompt surgical intervention is crucial in managing a strangulated femoral hernia containing an appendix [3]. Delayed diagnosis or treatment can lead to severe complications, including appendiceal perforation, peritonitis or even sepsis. Therefore, prompt surgical intervention is warranted.
Surgical strategies may vary depending on the surgeon’s expertise and patient-specific factors. The primary objective is to relieve the hernia’s strangulation and remove the appendix. This typically involves performing an appendicectomy and hernia repair concurrently. The choice between open or laparoscopic techniques depends on various factors, such as the surgeon’s preference, patient’s clinical condition and availability of resources. Dedopoulou et al. [4] reports to have performed an open femoral hernia repair and a laparoscopic appendectomy. Alternatively, Papatheofani et al. [1] reported to performing an appendectomy via a simple open approach.
Further literature search demonstrates another case study of a necrotic appendix where appendicectomy was performed through the hernia sac, followed by McVays technique to repair the hernia [5]. The varying surgical techniques reported demonstrate that there is no standard technique and management depends on the surgeon.
Postoperative management should focus on close monitoring of the patient’s recovery, including wound healing, pain management. Appropriate antibiotic therapy should be administered based on local protocols, especially if appendiceal perforation or infection is present [6]. Out-patient follow-up is essential in selective group.
The implications of a strangulated femoral hernia with an appendix extend beyond the individual case. Reporting such rare occurrences through case reports contributes to the existing medical literature, expanding the knowledge and understanding of this unique clinical entity. These reports facilitate improved diagnosis, management and decision-making for future cases. Moreover, they provide valuable insights into the prognosis, outcomes and potential complications associated with this condition.
In conclusion, a strangulated femoral hernia with an appendix represents a rare and diagnostically challenging clinical scenario. Timely recognition and prompt surgical intervention are essential to prevent potentially life-threatening complications. Collaboration among different specialties and continued reporting of such cases through well-documented case reports are crucial for further understanding and optimising the management of this unique presentation.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY
Data sharing is not applicable to this article as no new data were created or analysed in this study.

{kind=link}
{kind=link}