





Abstract
Peribulbar osseous choristoma is a benign, solid nodule; it is a subtype of epibulbar choristomas (belongs to single tissue choristomas), consisting of pure bony tissues. Epibulbar osseous choristoma is the rarest subtype of epibulbar choristomas, with only 65 cases reported since the mid-19th century; so, the rarity of the disease drove me to report it. A 7-year-old female presented with a painless left ocular superotemporal mass, which was present since birth and located under the conjunctiva. The primary diagnoses included lipodermoid and subconjunctival foreign bodies. Ocular interventions included a B-scan, examination under anesthesia and surgical excision of the mass in toto, and the histopathological examination showed that it was an osseous choristoma.
INTRODUCTION
A choristoma is a benign tumor made up of ectopic tissue that should be located somewhere else [1]. Epibulbar choristomas may impact the cornea, limbus and subconjunctival space, most often in the superotemporal region [2]. A solitary tissue choristoma (osseous tissue) on the sclera is known as an epibulbar osseous choristoma. Although epibulbar and ocular choristomas are common among children, osseous choristomas are extremely rare (the rarest type), with only 65 cases reported since Avon Grafe first characterized the lesion in 1863. Epibulbar choristomas develops from pluripotent mesoderm nests after birth. It was revealed that 69% of the patients were females, 76% of the lesions were in the right eye and 74% of the lesions were superotemporal [3–5]. There are four histological forms of epibulbar choristomas: dermoid, epidermoid, single-tissue choristomas and complex choristomas [6]. The lesion is usually asymptomatic and typically static and occurs sporadically in an otherwise normal eye [6, 7].
CASE REPORT
Chief complaint and history of present illness
An 8-year-old female patient presented with a left ocular mass that had been present since birth and started to enlarge, causing discomfort and a foreign body sensation. The family was worried about the nature of the mass. Regarding the systemic history, it was unremarkable. No history of ocular trauma or any other relevant history.
Examination
Visual acuity was 6/6 in both eyes, there was normal refraction in both eyes and intraocular pressure was 14 mmHg in the right eye and 12 mmHg in the left eye. Examination of the left eye showed a superotemporal subconjunctival mass, whitish in color, 10 mm from the limbus, ~6 × 6 mm in diameter and hard in consistency; the overlying conjunctiva was normal with dilated blood vessels surrounding the mass, as shown in Fig. 1. The provisional diagnoses were lipodermoid and a subconjunctival foreign body.
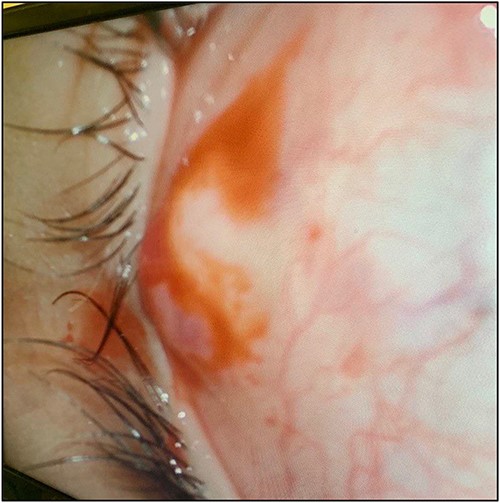
Picture showing the subconjunctival mass with overlying dilated vessels.
Treatment plan
The treatment decision was to excise the lesion, and informed written consent was obtained from the family to do the surgery. Surgical excision was performed under general anesthesia. The lesion was ~8 × 8 in diameter, whitish in color, hard in consistency and adherent to the conjunctiva, and underlying sclera but not to the muscles, as shown in Fig. 2A. The excised tissue was sent to the histopathologist, who revealed that the lesion is an osseous choristoma, as shown in Fig. 2B.
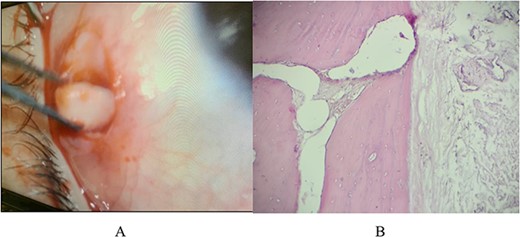
(A) Picture showing the gross anatomy of this white osseus lesion during removal from the subconjunctival space; (B) histologically the lesion was composed of mature lamellated bone with Haversian system and may be surrounded by thin connective tissues capsule, rarely some may have bony trabeculae with marrow elements.
DISCUSSION
Although it is most common in children, it has also been reported in adults. The lesion is usually congenital, although in certain cases, a history of trauma may be reported, which aroused attention. Surgery may be recommended to enhance eyesight, for esthetic reasons or to slow development. In addition, some lesions, especially the complex ones, are associated with a systemic condition such as Goldenhar’s syndrome [8].
A few of these lesions may be attached to the underlying sclera or extraocular muscles; nevertheless, the majority of osseous choristomas are tiny (<8 mm in diameter), firm to hard in consistency and have a swollen appearance [9]. Clinically, osseous choristoma has the following differential diagnoses: dermoid, herniated orbital fat, papilloma and dermolipomas [10]. Therefore, in most situations, histopathology is the sole technique available to confirm the diagnosis.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}