





Abstract
Retrocaval ureter (RCU) is a rare malformation of the inferior vena cava. We report a case of a 60-years-old female presented with right flank pain and computed tomography scan diagnosis of (RCU). She underwent robotic transposition and ureteroureterostomy of RCU. No complications were recorded. After 1 year of follow-up the patient remains asymptomatic and without signs of obstruction. Robotic repair of RCU with preservation of the retrocaval segment is a safe procedure with the advantages of the vision and dexterity in dissection and suturing.
INTRODUCTION
Retrocaval ureter (RCU) is a rare finding. Despite it was considered an urological disease, RCU is a congenital vascular anomaly of the inferior vena cava (IVC) characterized by course of a ureteral segment behind the posterior wall of the IVC with an incidence of 0.06–0.17% worldwide [1]. In case of hydronephrosis with recurring flank pain, upper urinary tract infection or progressive renal function loss, surgical management is the goal standard. Open, laparoscopic or robotic approaches have been described, but due to the rarity of this condition only case reports or few small series have been reported in the literature treated with robotic approach.
CASE REPORT
We report a case of a 60-years-old female, who came to our attention for persistent right flank pain and urinary tract infection. The computed tomography (CT) scan revealed right hydronephrosis with dilatation of the upper third of the ureter, up to L4, where it curved posteriorly to the IVC passing to its medial then anterior surface (Fig. 1). The 99mTc mercaptoacetyltriglycine (MAG-3) renal scan showed an obstructed pattern. After obtaining the patient’s consent, a robotic correction of the RCU was planned with the Da Vinci Xi. The patient was placed in lateral position. A pneumoperitoneum was created using a Veress needle, and the four robotic ports, spaced ⁓6 cm apart, were placed in a linear fashion on midclavicular line. Two ports for the assistant were placed at the lateral border of the rectus muscle. After the mobilization of the right colon to expose the retroperitoneal space, the ureter, the gonadic vain, the IVC and the renal pelvis were identified. After the transection of the ureter 3 cm below the ureteropelvic junction, the retrocaval segment was transposed anteriorly to the IVC and an ureteroureterostomy was performed with interrupted 4–0 monofilament sutures. After completion of the posterior layer, a 6F double J stent was insert in a retrograde fashion and the anastomosis was completed (Fig. 2). The operative time was 140 min, of which 90 min of console time. The post-operative stay was regular, the patient was discharged on post-operative day 4. The double J stent was removed after 30 post-operative days. After 1 year of follow-up the patient remains asymptomatic and imaging showed no signs of obstruction.
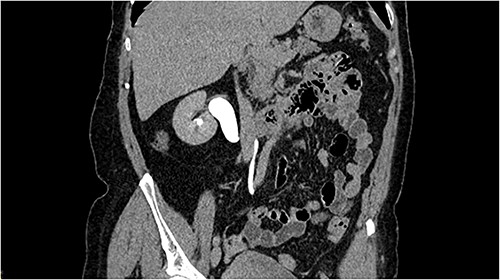
CT scan reconstruction with the image of the S-shaped ureter behind the IVC.
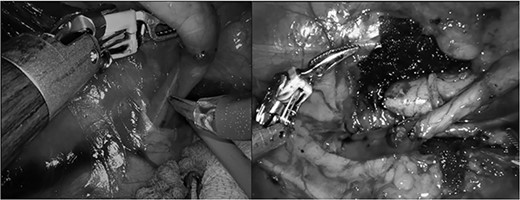
Intraoperative images of the ureter behind the IVC and after the transposition and the ureteroureterostomy.
DISCUSSION
The major data on outcomes of RCU treatment available in the literature concern open or laparoscopic approach. Two surgical techniques are most commonly used. The section of the ureter, with the retrocaval segment left in situ, and the subsequent ureteroureterostomy or the excision of the retrocaval segment to the IVC, with anteposition and ureteroureteral or ureteropelvic anastomosis. The classification, proposed by Bateson and Atkinson, of the RCU in two types guided the surgical choice. In type 1, the most common, the ureter shows as a fishhook or S-shaped ureter, as in our case, and the resection-anastomosis of the ureter, with the retrocaval segment left in situ, is the procedure of choice. In type 2, the obstruction is due to the compression of the IVC on a ureter that passes behind it; in these cases, uncrossing the ureter with restoration of continuity is the preferred technique [2]. These procedures are both efficacious, first one is simpler and faster, but may involve a risk of tension of the anastomosis. The second one, is more challenging for the risk of IVC injury, but it facilitates the anastomosis. In our case, we treated a type 1 RCU with preservation of the RCU, even if this technique is preferably used in type 2, where the ureter is not kinked behind the IVC. Despite the excision of the RCU is technically more difficult in our case, because it requires an extensive dissection of the IVC, this step facilitated the anastomosis. In our case, the robotic approach facilitated this operation. In the last years, small series of laparoscopic or robotic repair have been reported [2–5]. The longer operative time and the technical difficulties and the dexterity required for intracorporeal suturing in laparoscopic series are the major limiting factors compared to robotic approach [2–5]. Robotic approach with its three-dimensional view of the operative field and the EndoWrist technology has overcome these limitations [6]. Robotic repair of RCU with preservation of the retrocaval segment is a safe procedure.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest to declare.
FUNDING
None.
DATA AVAILABILITY
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.

{kind=link}
{kind=link}