





Abstract
Quadriceps tendon ruptures are common injuries, however isolated ruptures are rare. Particularly, reports for isolated vastus intermedius ruptures are very scarce. We present a case of a 62-years-old male patient who sustained a complete rupture of vastus intermedius tendon with a partial rupture of vastus medialis while rectus femoris tendon was intact, after a fall from standing height. Due to lag in extension, surgical treatment was performed, consisted of an end-to-end Krakow suture technique accompanied with two anchors placed on osseous attachment to the superior pole of the patella. A hinged knee brace locked in full extension was applied for 4 weeks. Gradual range of flexion was suggested after the 3rd postoperative week. Full range of motion was achieved in the 7th postoperative week.
INTRODUCTION
Rupture of the quadriceps tendon are common injuries, usually as the result of traumatic lesions leading to the disruption of the tendon insertion to the patella. Impairment of the knee extensor mechanism is often detected. Poor vascularization combined with the presence of degenerative distortions determine the higher incidence of such injuries in patients older than 40 years old [1]. The higher incidence has been observed through the 5th to 7th decade, since several systemic diseases have been identified to increase the risk of quadriceps tendon rupture due to tendon degeneration (diabetes, renal disease, hyperparathyroidism, rheumatoid arthritis, gout and collagen vascular disease and use of drug medications such as fluoroquinolone antibiotics and local or systemic steroids). Hence there are several reports of quadriceps tendon rupture without trauma, frequently following an eccentric overload on the tendon, especially in cases of a previous degenerative injury [2–4].
CASE PRESENTATION
A 62-year-old male presented to emergency department of our hospital with complaints of low back pain and decrease range of motion of the right knee due to a fall from standing height. The patient was unable to weight bear and to perform a straight leg raise. His past medical history revealed no significant records. Clinical examination revealed a low back pain without neurological deficit and tenderness at right knee with a palpable defect proximal to the superior pole of the patella. Passive flexion of injured knee was measured as 110° and passive extension was full. Routine laboratory tests including white blood cells (WBC) count, erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), liver and renal function were within normal ranges. The X-rays of the knee were normal without findings of patella baja and osseous pathology (Fig. 1), but the X-rays of the pelvis revealed bilateral sacroiliac arthritis. Based on this finding, further laboratory evaluation revealed a positive HLA-B27. An ultrasound scan performed externally showed a hypoechoic gap and quadriceps complete tear was noted. Magnetic resonance imaging (MRI) confirmed the findings seen on ultrasound with the difference that the rectus femoris (RF) was intact and there was a rupture of intermedius tendon (IT) combined with a partial rupture of vastus medialis. MRI sequences, especially T2W images revealed an intramuscular hematoma and discontinuity in the vastus IT (Figs 2 and 3). A small fluid filled defect, in the vastus intermedius just proximal to the insertion of quadriceps into the patella was also detected. The rectus femoris and vastus lateralis (VL) were intact. The defect in vastus intermedius measured ⁓5 cm from its patellar insertion.
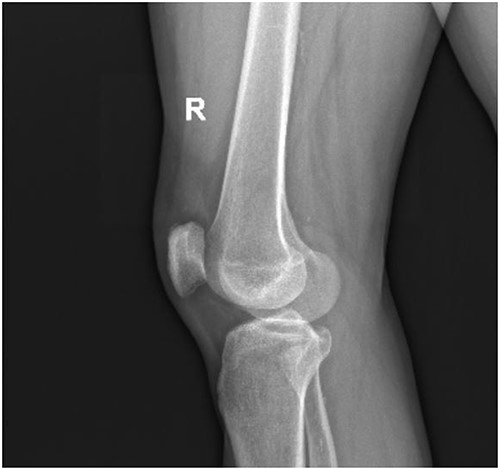
Lateral X-ray of the right knee without findings of patella baja and osseous pathology.

Fat saturated proton density sagittal view showing the rupture of the vastus IT with an intact rectus femoris tendon.
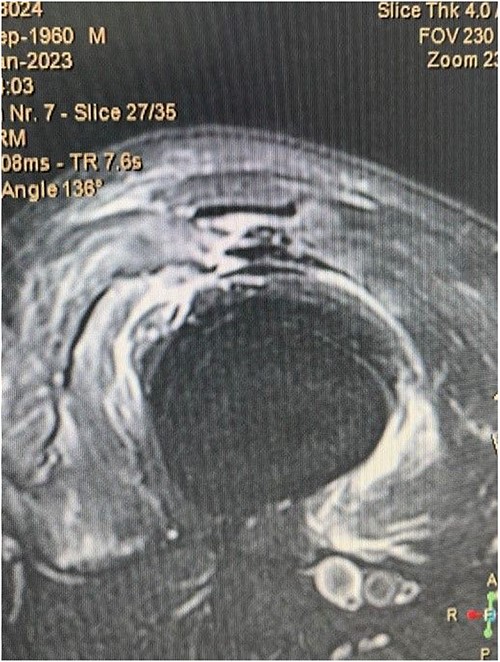
Fat saturated T2 axial view showing the rupture of vastus intermedius and vastus medialis tendon.
Surgical technique
Surgical repair was decided with a mid-axial longitudinal approach and full-thickness flaps were developed to avoid the damage to the skin blood supply. After the incision of the superficial fascia, the rectus femoris was intact and a medial suprapatellar incision was performed. The rupture of intermedius vastus tendon was confirmed with a concomitant partial rupture of the medialis vastus tendon. An end-to-end Krackow sutures were placed through the intermedius vastus, associated with two anchors which were implanted into the patella after drilling and two pairs of nonabsorbable sutures were placed through the intermedius vastus tendon via the same Krakow technique. An end-to-end Ethicon sutures were placed through the vastus medialis tendon.
Rehabilitation progress
Following surgery, a hinged knee brace locked in full extension was applied for 4 weeks to protect tendon repair. In the 5th and the 6th week, 30 and 60° of flexion were allowed, respectively. Further flexion range until 90° was allowed and full range of flexion gradually achieved in the 7th week. After 1 week the brace was removed and range of motion exercises, eccentric exercises, stretching and proprioception exercise programs were performed. Partial weight bearing allowed after the 3rd week, followed by full weight bearing at the 6th week. The brace was removed at the 8th week.
DISCUSSION
Quadriceps tendon ruptures are usually consist of full-thickness tears of the trilaminar layered extensor mechanism to its osseous insertion in the superior pole of the patella. Partial ruptures are rare, thus reports in the literature are scarce [5]. Moreover, partial tears are more commonly detected in the vastus IT, while complete tears are more frequently incurred in the VL, vastus medialis and rectus femoris [6].
Both clinical and perioperative detection of isolated VI rupture are difficult due to the overlaying intact RF [7]. The diversity of the quadriceps tendon anatomy may determine the potential partial or full-thickness tear, since several layers of attachment have been identified [8, 9]. Given that, MRI is the mainstay imaging modality for both partial or complete rupture detection and treatment guidance. Moreover, despite MRI, a palpable defect proximal to the superior pole of the patella, combined with an inability to perform a straight leg raise (loss in extension), should raise the suspicion of an underlying tear. Also, real-time dynamic scanning can provide significant diagnostic guidance; hence ultrasound constitutes the first diagnostic process in several cases. However, the diagnostic facility of ultrasound in partial ruptures is not established [7, 10].
The relatively rare incidence of isolated ruptures of VI determines the scarce literature reports and the lack of enough evidence considering the optimal management of such patients. To our knowledge only three studies have reported an isolated rupture of the VI with an intact RF. Thompson et al. presented three cases of isolated VI rupture where both surgical and conservative management were performed. The authors report a lag of extension in all patients combined with an MRI confirmed isolated rupture of VI. Conservative treatment was applied in one case since severe time elapsed from injury to diagnosis, while surgical repair was performed in two patients, one of whom submitted to a revision procedure due to re-rupture [7]. On the other hand, Cetinkaya et al. and Azzopardi et al., have both reported the conservative management of patients with isolated VI rupture [5, 11]. Regardless of surgical or conservative management, a hinged knee brace was applied in all cases. Full range of motion and partial weight bear is allowed after the 3rd or 4th week followed by stretching and proprioception physiotherapies after the 6th week. Functional rehabilitation process is sufficient in both cases of surgical or conservative treatment since a post-treatment physiotherapy protocol is applied [5, 7, 11].
The deficiency of an established definitive treatment for isolated VI tears is attributed to the limited reports owing the scarce incidence of such injuries. To our opinion, given the satisfying outcome of both management procedures, the range of the extensor mechanism defect should be greatly considered as far as the surgical intervention is concerned. As we have already pointed out, regardless of the type of management, an MRI is warranted to identify the tear pattern and optimize the potential surgical plan. Where surgical procedure is demanded, repair withing 48 h should be performed to reduce morbidity and decrease the risk of surgical failure [7, 12].
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no actual or potential conflict of interest in relation to this article.
FUNDING
All authors have declared that no financial support was received, and they have no financial relationships at present or within the previous years with any organization that might have an interest in the submitted work.
DISCLOSURES
The study was approved by the Scientific Committee of our hospital. Written consent was obtained by the patient to participate in this study.
DATA AVAILABILITY
The study was approved by the Scientific Committee of our hospital. Written consent was obtained by the patient to participate in this study.

{kind=link}
{kind=link}
{kind=link}