





Abstract
Hybrid surgery (abdominal robotic approach with a trans-anal approach) has been reported to improve oncological outcomes in cases involving advanced cancer or technical difficulties. A 74-year-old woman presented with anal pain and stenosis. Examination revealed palpable sclerosis on the anterior wall at the anal verge with possible vaginal invasion. A biopsy revealed an adenocarcinoma. We performed a two-team robot-assisted abdominoperineal resection combined with resection of the vagina supported by a simultaneous trans-perineal approach. After rendezvous at the posterior side, the abdominal team cut the posterior wall of the vaginal vault while the perineal team confirmed the surgical margin. Histopathological findings identified the tumour as an anal gland adenocarcinoma (pT4b [vagina] N0M0 pathological stage IIC) with a negative circumferential resection margin. Hybrid surgery combined with resection of the posterior wall of the vagina may be performed safely and is a valuable surgical option for multimodal treatment of anal adenocarcinomas.
INTRODUCTION
Robot-assisted total mesorectal excision (TME) and trans-anal TME (TaTME) are important surgical strategies for rectal cancer [1, 2], with advantages for improving oncological and functional outcomes [1–3]. Hybrid surgery, which comprises an abdominal robotic approach with TaTME, has been reported as a novel strategy for securing surgical margin in cases involving advanced cancer or technical difficulties [4, 5]. Herein, we describe a case of hybrid robot-assisted abdominoperineal resection (APR), supported by the trans-perineal approach, for anal gland adenocarcinoma with vaginal invasion.
CASE REPORT
A 74-year-old woman presented to our department with anal pain and stenosis. Digital examination revealed palpable sclerosis on the anterior wall at the anal verge. Although the tumour was not exposed on the vaginal mucosa, a dent on the posterior wall of the vagina suggested vaginal invasion. Because a previous biopsy performed using colonoscopy specimens was negative, a trans-anal biopsy was performed under lumbar anaesthesia. Histopathological examination revealed an adenocarcinoma. Computed tomography did not reveal enlarged lymph nodes or distant metastases. Thus, the preoperative clinical TNM stage was determined to be T4b (vagina) N0M0 (clinical stage IIC). We performed a two-team, robot-assisted APR combined with vaginal resection supported by a simultaneous trans-perineal approach. The operating room settings are illustrated in Fig. 1. The robot-assisted TME was performed using the da Vinci® Xi Surgical System (Intuitive Surgical Inc., Sunnyvale, CA, USA). The trans-perineal approach was applied using EZ access™ with a LAP PROTECTOR mini™ (Haako Co. Ltd, Nagano, Japan) and an AirSeal® System (ConMed, Utica, NY). The abdominal team (robot-assisted approach) performed mobilization of the sigmoid colon by medial-to-lateral approach and ligated the root of the inferior mesenteric artery. Simultaneously, after the perineal team (trans-perineal approach) connected the perineal skin incision to the posterior side of the vagina, they performed a purse-string suture on the perineal skin and attached an EZ access. The perineal team mainly dissected the lateral and posterior sides around the anal canal. TME up to the levator ani muscle was performed by the robot-assisted approach. After dissecting levator ani muscle, ‘rendezvous’ (indicating that the two dissection teams met) was achieved at the posterior side. At the anterior side, the abdominal team opened the peritoneal reflection and cut the posterior wall of the vaginal vault while the perineal team confirmed the surgical margin of the tumour (Fig. 2). Finally, both teams dissected the lateral sides. The TME was completed under the pneumoperitoneum, and the specimen was removed from the perineal incision. The defect in the posterior vaginal wall was reconstructed by simple closure using an absorbable thread, and the perineal wound was closed primarily. The operation time was 286 min, and the blood loss volume was 100 mL. A macroscopic photograph of the specimen is shown in Fig. 3. Microscopically, tumour cells were observed to mainly infiltrate the submucosal layer to the vaginal wall (Fig. 4a). The tumour cells were positive for cytokeratin (CK) 7, caudal-type homeobox 2 (CDX2), and mucin 5 subtype AC (MUC5AC), but negative for CK20 (Fig. 4b–e). Based on histopathological findings, the tumour was diagnosed as an adenocarcinoma of the anal glands (pT4b [vagina] N0M0 pathological stage IIC; negative circumferential resection margin [2 mm]). The patient was discharged 8 days after the operation without complications and is currently undergoing adjuvant chemotherapy.
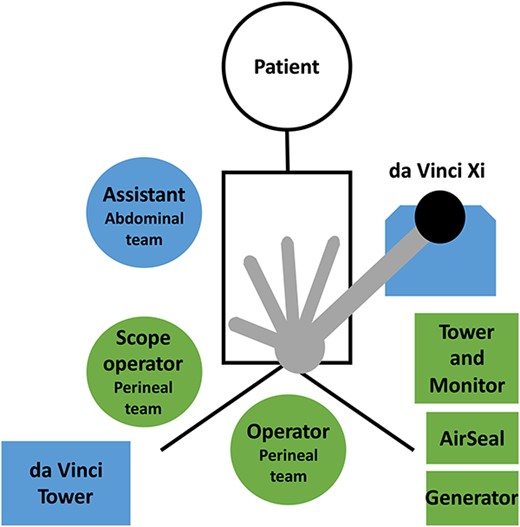
The operating room settings for the hybrid surgery. The da Vinci Xi is rolled from the left side of the patient. The assistant in the abdominal team is positioned on the right side of the patient. The operator in the perineal team is positioned between the patient’s legs. The scope operator stands on the outer side of the right leg. The tower and monitor, AirSeal, and generator in the perineal team are located on the left side of the patient and on the caudal side of the da Vinci Xi.
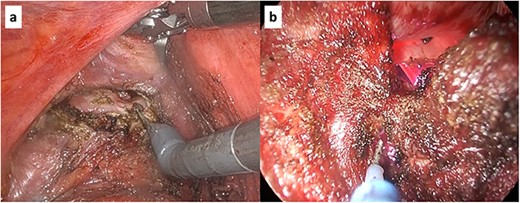
Intraoperative findings in hybrid surgery. (a) Robot-assisted approach. (b) Trans-perineal approach. The two photographs show the dissection of the posterior wall of the vagina.
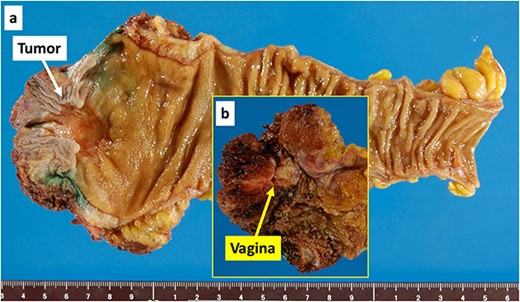
Macroscopic photograph of the specimen. (a) The tumour indicated by the white arrow was a Type 3 tumour measuring 25 × 25 mm. (b) The photograph in the yellow window shows the dissection surface. The yellow arrow indicates the resected vagina.
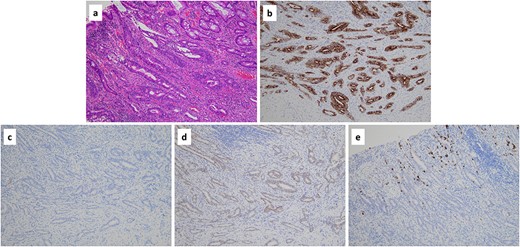
(a) Histopathological findings revealed an adenocarcinoma based on haematoxylin and eosin staining (×10). (b-e) Immunohistochemically, the tumour was positive for cytokeratin 7 (×10) (b), negative for cytokeratin 20 (×10) (c), positive for caudal-type homeobox-2 (×10) (d) and focally positive for mucin 5 subtype AC (×10) (e).
DISCUSSION
In the present case, we performed a hybrid surgery (robot-assisted APR supported by simultaneous trans-perineal approach) for an anal gland adenocarcinoma with vaginal invasion and achieved a successful operation with accurate surgical margins. Recently, minimally invasive surgery (MIS) is preferred in locally advanced colorectal cancer [6]. Although combined adjacent organ resection for rectal cancer is difficult because of high mobility [7], recent developments in MIS including robot-assisted surgery have facilitated combined resection of other organs [8, 9]. Especially, robot-assisted rectal surgery could be useful for the combined resection of the uterus or vagina in women such as the present case, because the vaginal vault can be cut more easily and accurately owing to increased manoeuvrability by multiple joints [9]. Furthermore, the pneumoperitoneum was maintained even after the rendezvous using a simultaneous trans-perineal approach; hence, we proceeded to complete the dissection while confirming the accurate surgical margin under magnification (Fig. 5). Oshio et al. [5] reported that hybrid trans-abdominal robotic surgery and TaTME was performed safely and may improve oncological outcomes by achieving a negative resection margin for rectal cancer. However, because there have been still few reports on this surgery [4, 5], hybrid surgery is considered to be a novel surgical approach. We consider that hybrid surgery is a feasible surgical technique for anorectal cancer and this case is a good candidate for hybrid surgery.
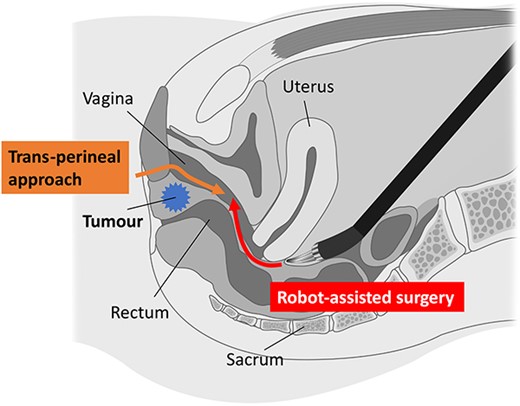
Schema of hybrid surgery. In robot-assisted surgery, the cutting of the vaginal vault can be performed more easily and accurately owing to multi-joint manipulation. The simultaneous perineal approach confirmed the surgical margin of the tumour under magnification.
Primary anal gland adenocarcinoma is rare. Primary anal canal adenocarcinomas are classified as intestinal, anal gland, fistula-associated, and non-anal gland- and non-fistula-associated adenocarcinomas [10]. Anal gland adenocarcinoma typically occurs as an intramural adenocarcinoma with an unaffected overlying anorectal mucosa [11]; it is characterized by CK7 and MUC5AC positivity and CK20 or CDX2 negativity [10]. Hobbs et al. [12] proposed the following definition of anal gland carcinomas: tumours composed of haphazardly dispersed CK7-positive small glands with scant mucin production, invading the wall of the anorectal area, without an intraluminal component. Our case met these criteria. Owing to the rarity of anal gland adenocarcinomas, a standard treatment has not been established [13, 14]. However, Anwar et al. [13] concluded that the optimal treatment is a combination of radical surgical resection and neoadjuvant or adjuvant treatment. Furthermore, early diagnosis of anal gland adenocarcinomas is difficult because mucosal involvement at the onset is unlikely [11]. Therefore, extended surgical resection is required [15], which was performed in our case, to secure the surgical margin. Hybrid surgery can be an option for such an extended surgery. The optimal surgical approach is an issue for further study.
In conclusion, hybrid surgery combined with resection of the posterior wall of the vagina was performed safely for an anal gland adenocarcinoma with vaginal invasion. This procedure can be a surgical option in a multimodal strategy for anal canal adenocarcinomas.
ACKNOWLEDGEMENTS
We would like to thank Dr Tatsuo Kyuno (Suginami Proctology Clinic) for performing the patient follow-up.
CONFLICT OF INTEREST STATEMENT
All authors declare they have no conflict of interest.
FUNDING
This report did not receive any grant or financial support.
DATA AVAILABILITY
The data that support the findings of this report are available on request from the corresponding author.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE AND PUBLICATION
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}