





Abstract
Myxomas are rare neoplasms of mesenchymal origin, which consist of many undifferentiated stellate and spindle-shaped cells in abundant loose myxoid stroma with collagen fibers. A 74-year-old patient presented in our oral and maxillofacial department with a slow growing mass within the upper lip. The mass was surgically excised in the toto, followed by a histological and immunohistochemical examination. The findings revealed that it was a myxoma. These tumors are very rare and should be included in the differential diagnosis of damage of the upper lip. As long as the myxoma is properly removed, there is no risk of recurrence.
INTRODUCTION
Virchow was the first to describe a neoplasm in 1871, which consisted of a mucoid substance the same as in the umbilical cord [1]. Myxomas are rare neoplasms of mesenchymal origin, which consist of many undifferentiated stellate and spindle-shaped cells in abundant loose myxoid stroma with collagen fibers. Mucopolysaccharides and glycosaminoglycans such as hyaluronic acid and chondroitin sulfate can also be found. Immunohistochemically, antibodies directed against proteins such as vimentin and actin are very characteristic [2]. Unlike its odontogenic origin counterpart (odontogenic myxoma), which arises primarily from odontogenic ectomesechyma, and it is mostly found in the maxilla and mandible, soft tissue myxomas are rare in the head and neck region [3]. More specifically, they account for <1% of soft tissue tumors (0.12%) in the human body [4]. They can affect tissues such as skeletal muscles, especially muscles of the thigh, the adductors, gluteus, gastrocnemius and the upper arm. The heart muscle is also frequently affected, mostly the heart valves [5]. Furthermore, myxomas can also arise within bones other than the splanchnocranium complex such as the femur, the clavicle and the metatarsal bones, but such situations are very rare [5]. To the best of our knowledge, only a few cases of soft tissue myxomas were found in the oral cavity, mostly in regions such as the buccal mucosa, lips, gingiva and palate. We found 38 cases of myxomas in the mouth after a brief literature review from 1908 until 2020, from which only 6 cases can be located in the soft tissues of the lips. As far as we can notice, our case resembles the seventh myxoma documented in the upper lip.
CASE REPORT
A 74-year-old patient presented in our oral and maxillofacial department with a slow growing mass within the upper lip.
The medical and dental histories were unremarkable, except for multiple extractions of upper teeth due to periodontitis. The lesion first appeared about 2 years ago, but started enlarging during the past 6 months. The patient had difficulty eating and drinking, but had no pain complaints. During the clinical examination, the mass was soft and mobile at palpation, not tender and well demarcated in the upper lip and labial vestibule (Fig. 1A and B). The overlying mucosa was normal with no signs of inflammation, except for a small area of tissue that presented with a leukoplakia, possibly because of irritation. Examination of the panoramic radiograph showed no signs of bone involvement. The differential diagnosis of a mass in the upper lip included soft tissue neoplasms (lipomas, fibromas), salivary gland neoplasms (pleomorphic adenoma and canalicular adenoma) and irritation fibroma. Mucoceles could also be involved, but they are more common in the lower lip. An excisional biopsy was performed under general anesthesia. Topical use of articaine 4% with epinephrine 1:200 000 was used to obtain pain control and vasoconstriction. An incision along the overlying mucosa with a #15 blade was carried out at the maximum convexity of the lesion. This was followed by blunt dissection of the soft tissue around the mass, which was very easily separated from the adjacent structures. Clear margins of normal tissues were achieved (Fig. 2A–D). With the use of 4–0 resorbable sutures, primary closure was achieved, and the patient followed the post-surgical instructions. Monthly follow-up showed good healing with no signs of recurrence.
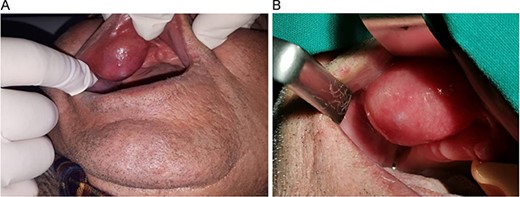
(A & B) Proper retraction of the upper lip shows the extension of the masss in the bucco-labial vestibule.
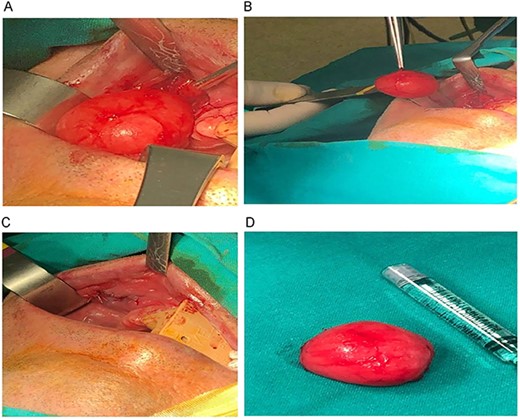
(A–D) Sequence of the surgical procedure.
The surgically extracted in the toto mass was oval-shaped with a myxoid appearance, soft during palpation and yellowish in apperance. It was 3.2 cm at its greatest diameter. The mass was histologically and immunohistochemically examined (Figs 3–5). The tumor was severely hypocellular and consisted of stellate and spindle cells without atypia or mitosis, in an abundant myxoid stroma. Immunohistochemically, the tumor cells were positive for vimentin and CD34 but negative for SMA and S100. Based on these findings, a myxoma diagnosis was made.
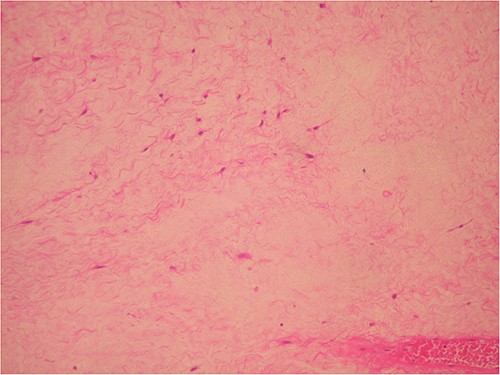
Severe hypocellular tumors. Stellate and spindle cells in abundant myxoid stroma (H & E ×100).
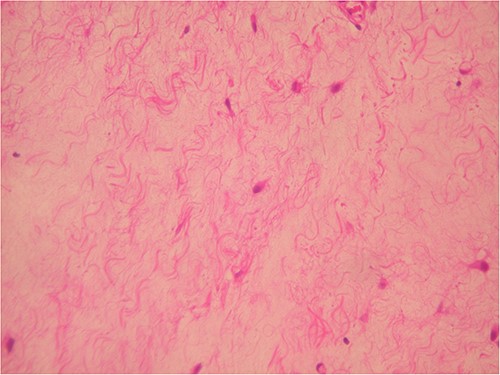
The same area in higher magnification (H & E ×200).
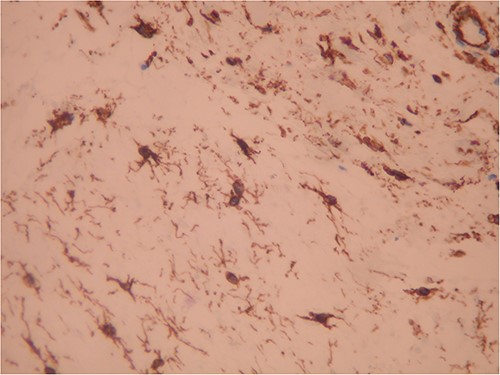
Strong positivity for CD34 of tumor cells (IHC ×200).
DISCUSSION
Myxomas are very rare in the oral cavity. Our review of the literature revealed 38 cases of myxomas in the oral region. They are located in the gingiva, the palate, buccal mucosa, floor of the mouth, retromoral region and the lips. The occurrence frequency of myxoma in the gingiva is about 13.1%, palate 34.2%, the bucca mucosa 21%, the floor of the mouth 5.2% and the lip 15.7% [6–9].There are only six cases of myxomas in the lips and we present the seventh case located in the upper lip. Andrews et al. also described two cases of myxoma in the mandible:one in the maxillary sinus, one in the sphenoid sinus and one in the parotid gland [5]. Ramaray et al. described a case of myxoma in the soft tissue of the maxilla, and Ye et al. described a myxoma of the temporomandibular joint [10, 11].
CONCLUSION
Myxoma constitutes a rare tumor that should be included in the differential diagnosis of damage of the upper lip. When the tumor is excised properly, there is usually no recurrence.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY STATEMENT
All authors provide a data availability statement in their manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}