





Abstract
An epidermoid cyst is a common benign cutaneous mass that mostly occurs on the neck, face and trunk. The majority of epidermoid cysts are small and asymptomatic with the giant perineal epidermal cyst being rare and more liable to develop complications such as malignant transformation. The treatment of an epidermal cyst involves total excision of the cyst along with its wall to prevent recurrence. We present an unusual case of a giant perineal epidermal cyst in a 52-year-old male.
INTRODUCTION
An epidermoid cyst is a developmental cyst that may arise as a result of entrapment of a pluripotent cell or implantation of an epithelium [1]. Most epidermoid cysts are small, benign, and asymptomatic, occurring intradermally or just below the skin. Cysts measuring >5 cm in diameter are a rare occurrence that is referred to as giant epidermoid cysts. Such big cysts are prone to complications such as intracyst hemorrhage and malignant transformation, mostly squamous cell carcinoma (SCC) with an incidence of 0.011–0.045% [2, 3].
This kind of cyst is usually seen in the chronic sun-exposed areas of the skin including the face, neck or trunk with perineal and extremity locations being rare [1, 4]. The prevalence is twice as common in males compared with females and can be diagnosed at any age but more commonly seen in the third and fourth decades of life [5]. We present a rare case of a giant benign perineal epidermoid cyst in a 52-year-old male who was successfully treated by surgical excision.
CASE REPORT
We present a case of a 52-year-old male patient who was diagnosed with a complaint of a painless perineal mass for 3 years. The mass was progressively increasing in size with time and was associated with difficulties in siting and walking. He denied a history of having lower urinary tract symptoms, fevers, difficulties in defecation, prior perineal surgery or trauma. In addition, he denied any history of cigarette smoking or contracting a human papilloma virus infection. He was attended at a nearby health facility and kept on some oral medication that he combined with some local herbs, but there was no improvement; instead, the swelling kept on increasing in size slowly. Later on, he was referred to our health facility for a second opinion.
The examination of the external genitalia and perineum revealed normal male external genitalia with shaved pubic and perineal hair.
Both testes were palpable within their respective hemiscrotal sacs and were normal in size and consistency. There was a well circumscribed, smooth surface, freely mobile, firm, non-tender, roundish midline mass on the perineum with normal overlying skin. The mass measured approximately 7 cm × 9 cm (Figs 1 and 2). However, there was no induration felt on the perineum. A working diagnosis of a perineal pilonidal cyst with the differential diagnosis of perineal lipoma and infected hair follicle was entertained. Full blood count, urinalysis, serum creatinine and random blood sugar were within normal limits. The ultrasonography of the mass revealed a well-emarginated ovoid mass with echogenic contents.

The perineal mass involving the lower aspect of the scrotum and perineum (an arrow), separately from the testis (blue dots).

The mass marked by an arrow was separate from the testis (blue dots), which are pushed cephalad by the examiner’s gloved index finger.
The patient underwent an en bloc surgical excision of the perineal mass together with the overlying skin (Figs 3 and 4) followed by primary closure of the wound (Fig. 5). The mass that weighed 228 g (Fig. 6) was removed and sent for histopathological evaluation, which confirmed the diagnosis of an epidermoid cyst as it consisted of stratified squamous epithelium that was lined with a granular layer with abundant keratin flakes (Fig. 7).
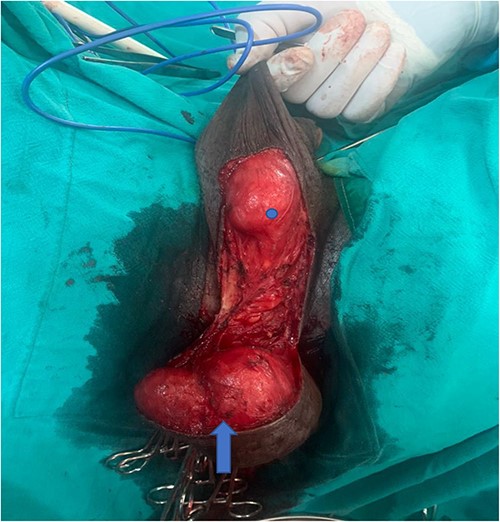
Lobulated mass (blue arrow) is adherent to the perineal skin and part of scrotal skin. One of the testes (blue dot) can be seen separate from the mass.

The excised mass.

Image showing a primary wound closure in a Y-fashion.
The weight of the mass in grams.
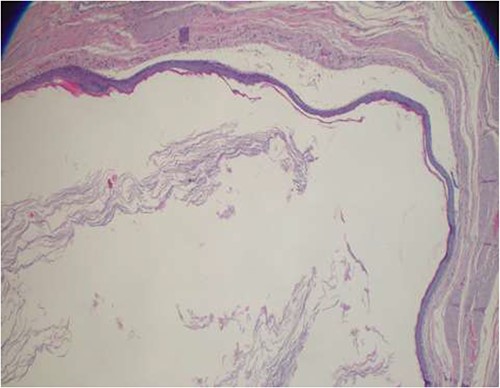
Photomicroscope highlighting a stratified squamous epithelial lining with a granular layer and abundant keratin flakes filling the cystic cavity (hematoxylin and eosin-stained sections, ×40 original magnification).
The patient had an uneventful recovery postoperatively and has been followed up closely. The last time he was seen at the clinic was at 8th month postoperatively and he had no complaints. Perineal examination revealed healed surgical incision with no evidence of recurrence.
DISCUSSION
Epidermoid cysts are approximately twice as common in men as in women. They may occur any time in life, but they are more common in the third and fourth decades of life. Our case was a male patient in his fifth decade. They are commonly distributed all over the body but uncommonly reported in the perineum [1]. Risk factors include exposure to ultraviolet rays, human papilloma virus infection, smoking and trauma [4]. Specific risk factors for perineal epidermoid cyst include mechanical pressure, perineal surgery, needle biopsies and minor trauma on the perineal area [3].
Epidermal cysts are usually asymptomatic; however, symptoms may arise if they become infected or very large. The malignant transformation of epidermal cysts is very rare. In particular, perineal SCC arising from an epidermoid cyst is extremely rare, and to date, very few cases have been reported in literature [3]. The differential diagnoses of perineal epidermoid cysts are lipoma, abscess, pilonidal cyst, dermoid cyst, soft tissue tumors such as benign teratoma and skin cancer [4]. Clinically, it is often difficult and almost impossible to differentiate benign from malignant perineal cystic lesions. It is important to distinguish between perineal abscess, which is a common clinical condition, and an infected perineal cyst, an uncommon disease because incision and drainage are sufficient for abscess, whereas complete excision is required for an infected perineal cyst [4]. Currently, magnetic resonance imaging (MRI) is the investigation of choice that helps to rule out a number of differential diagnoses [5]. The cyst shows low and intermediate/high signal intensity on T1- and T2-weighted MRI images, respectively. This cysts tend to have a high signal intensity on fat-saturated images with thin peripheral enhancement and significant diffusion restriction [4]. In our case, however, MRI imaging was not done because of not only financial constraints but also that by the time the patient came to our health facility, the examination was not available at the center. On ultrasound, epidermoid cyst usually exhibits a thick-walled ovoid or roundish mass with echogenic debris, and sometimes, one might observe multiple dependent echogenic nodules within the cystic mass [4]. Similarly, in our case, the ultrasound revealed a roundish cyst that contained echogenic material. However, due to the operator dependency of ultrasound, we missed a number of information regarding the mass and we believe that it may not be a very good test for this kind of mass.
Histologically epidermoid cysts are lined by a stratified squamous epithelium containing a granular layer that is filled with keratin material. These features make the confirmatory diagnosis of an epidermoid cyst [5]. The aforementioned characteristics are in keeping with the histological finding in our case. Although large cysts have been linked to malignant transformation, the index case was benign.
The treatment of choice for an epidermoid cyst is a complete surgical excision of the entire cyst and its wall with wide free margins. The postoperative prognosis is excellent as the chance of recurrence is very low (3%) [5]. Our patient had a good prognosis with no evidence of recurrence at 8 months postoperatively.
CONCLUSION
A perineal epidermal cyst is a rare clinical entity and should be considered as one of the differential diagnoses of perineal masses. Regardless of its size, an en bloc surgical excision of the cyst is the preferred treatment of choice with a good outcome.
ACKNOWLEDGEMENTS
We would like to thank the patient for his acceptance and permission in sharing and publication of this case report. We would also like to acknowledge all urology staff members who were involved in the care of this patient.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
This work has not received any funds from any individual or organisation.
CONSENT
The authors declare that the patient consented for his images and the whole history to be published, and we will make sure that his identity including his name will not be used anywhere in the writings.
AUTHORS' CONTRIBUTIONS
M.K., O.J.M., F.B., M.S. and B.N.N. were involved in the surgery, managed the patient pre- and post-operatively, and wrote the initial draft of the case report. A.M. was involved in the histopathological evaluation of the mass. M.K. and O.J.M. wrote the initial draft. B.N.N., A.K.M., M.S., J.S.M. and A.K.M. reviewed the initial draft.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}