





Abstract
Tracer site hernias (TSHs) are extremely uncommon. There have been only a few cases reported in the literature. Here we report a case of TSH after umbilicus laparoscopic hernia repair procedure. Diagnosis was based on patient symptoms and computed tomography. Patient underwent exploratory laparoscopy followed by laparoscopic hernia repair with mesh. We also provide a mini review of the literature in order to highlight that although rare, this pathology should be included in the differential diagnosis of acute abdomen.
INTRODUCTION
Laparoscopic approaches have gained widespread acceptance due to minimal invasive advantages. Small incisions, shorter hospitalization and decreased complication rate, are the most frequent. Despite of laparoscopy safety, some complications could be occurred. A very uncommon complication after laparoscopic procedures, is tracer site hernia (TSH), ranging between 0.5 and 2% [1, 2]. TSH has been known since 1987. TSH can cause small bowel obstruction, which can lead to emergency surgery [1]. TSH has been occurred most often in trocar sites of a minimum 10 mm in diameter and located mostly in the umbilicus region [2]. In this paper, we report a case of a TSH that caused acute abdominal pain in a female patient, as a result of part small bowel herniation. A review of the literature considering this rare entity is also performed.
CASE REPORT
A 48-year-old woman was admitted to our department in order to have laparoscopic repair for a symptomatic umbilical hernia. The patient suffered for allergic asthma. Three ports were inserted, two 10-mm ports at the left lateral abdomen, and one port 5 mm at the right lateral abdomen. The next day the patient was discharged with no complications. The second postoperative day the patient reported diffuse abdominal pain, constipation, nausea and vomiting. An abdominal X-ray was carried out, without any useful information. Abdominal computed tomography revealed the small bowel herniation (Fig. 1a) through the 10-mm trocar at the left lateral abdomen (Fig. 1b).
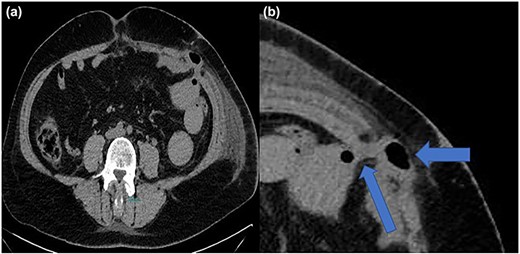
(a, b) Computed tomography imaging with TSH and intestinal involvement (blue arrows).
Because of extreme pain and symptom of ileus, a laparoscopic exploration was performed. Laparoscopy confirmed the small bowel herniation in the fascia defect (Fig. 2). The small bowel was captured with an intestinal grasper and repositioning in the abdominal cavity. Then the dehiscence of the fascia was closed with individual absorbable sutures and with semi-absorbable round mesh 6.4 cm in diameter (Ventralex Bard). The small bowel was no ischemic and immediately we recognize peristalsis. The patient after surgery was revealed of her symptoms and she was mobilized the same day. She remained stable throughout her hospitalization and the third postoperative day was discharged. The follow-up lasted for 30 days in our outpatient department.
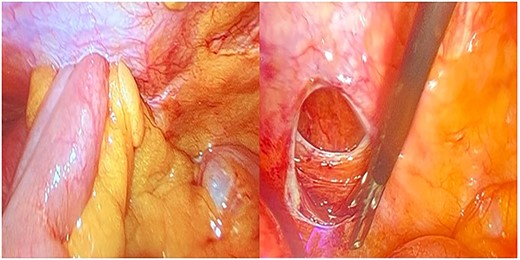
Intraoperative findings before and after hernia repair.
DISCUSSION
TSH is a serious complication after laparoscopic procedures, as it can lead to life-threatening complications, such as small bowel obstruction and strangulation. By this case we can understand the necessity to investigate any complaint postoperatively.
Fear was the first in 1968 that report a TSH in his large series of laparoscopic gynecological procedures. Maio and Ruchman the reported a TSH with small bowel obstruction immediately after cholecystectomy. Since then many reports and meta-analyses have been published about TSH [3].
Patients with a TSH presents with nausea, vomiting, abdominal pain and abdominal mass usually a few days after a laparoscopic procedure. If a TSH is suspected, a CT scan can be helpful for diagnosis, which can not only find the herniation site, but also define its classification.
The TSH occurs more often at the umbilical trocar due to the larger trocar placement for this region. Despite this fact, in the last decades a few case reports represent the TSH at the lateral site trocar. These hernias have been associated with early onset of the symptoms of the patient, which often require an emergency surgery [4].
Many risk factors have been associated with the occurrence of TSHs, which are distinguished into patient-related and surgery-related. The patient-related risk factors include age > 60 years, BMI > 28 kg/m2, surgical infection, uncontrolled diabetes mellitus, previous abdominal surgery and smoking. The surgery-related risk factors include prolonged surgical duration, trocar size, the region of trocar placement, non-closure of the fascia and trocar type. [5–8].
TSH is rare but also a life-threating complication. Postoperative instructions should be given to all patients, undergone minimal invasive procedures. Patients should be avoiding activities, which increase the abdominal pressure for at least 2 weeks postoperatively [9].
Follow up of all patients is crucial even in case of minimal invasive procedures. Evaluation of every postoperative complaints is important. High clinical suspicion, especially in patients with risk factors. According to last guidelines of European and American hernia society, recommended to suture the fascial defect for trocar sites of 10 mm or larger, especially in umbilicus area. Lately, in the literature is recommended to close 5-mm defects in the fascia in case of multiple risk factors and prolonged minimal invasive procedures [8–10].
ACKNOWLEDGMENTS
Authors would like to appreciate the Papageorgiou Foundation.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}