





Abstract
Horseshoe kidney is the most prevalent congenital kidney fusion anomaly, affecting 0.25% of the general population and occurring in 1 in 400–1600 births. Approximately 40 percent of patients develop kidney stones due to anomalies. In our case, we aimed to perform combined laparoscopic pyelolithotomy with retrograde intrarenal surgery (RIRS) instead of percutaneous nephrolithotomy (PNL) in a patient with a horseshoe anomaly. This procedure enabled us to detect the location of the mobile stone with RIRS and then successfully extract it with laparoscopic pyelolithotomy. Laparoscopic pyelolithotomy combined with RIRS is a reasonable additional treatment option for complicated stone surgery due to horseshoe kidney anomalies.
Introduction
The horseshoe kidney anomaly, the congenital fusion defect of the kidneys, has an incidence rate of around 0.25% in the general population and is observed in roughly 1 out of every 400–1600 births [1]. The incidence of this condition is higher in males by a ratio of 2:1 compared with females. In most cases, fusion occurs at the kidney’s lower pole. This results in abnormalities in the kidney’s position, rotation, and vascular nutrition. Horseshoe kidney may result in urine stasis and stone development due to poor drainage of the collecting system and obstruction at the ureteropelvic junction [1].
Urolithiasis is the most frequent complication of horseshoe kidney, manifesting in 20%–60% of cases [2]. Percutaneous nephrolithotomy (PNL), extracorporeal shock wave lithotripsy (ESWL), flexible ureteroscopy (f-URS), laparoscopic, robotic, and open procedures have been used to treat horseshoe kidney stones [2]. Due to the frequent presence of concomitant anatomical, vascular, and positional anomalies, there is no standardized approach to the treatment of horseshoe kidney stones [2]. The standard treatment approach described in the literature needs to be established, particularly when the stone exhibits mobility.
This case report presents our operation with a combined laparoscopic pyelolithotomy and retrograde intrarenal surgery (RIRS) in a patient with a horseshoe kidney anomaly and a mobile kidney stone.
Case presentation
A 24-year-old male patient presented with a complaint of left flank pain. The patient complained of intermittent pain for 5 years and had no prior history of kidney stones or hematuria. As shown in Fig. 1(A and B), during the non-contrast computed tomography (CT) scan of the entire abdomen conducted 5 months ago, a horseshoe kidney anomaly was detected in the patient. At the same time, a 22-mm stone localized to the collecting system at the level of the kidneys with fusion in front of the aorta and a 6-mm stone located in the middle part of the left kidney were found. Subsequent evaluation revealed that the stone had moved and settled in the left renal pelvis. Due to the renal anomaly, any leftover fragments following RIRS will not spontaneously fall out because the stone is mobile between the lower calyx and the renal pelvis. Therefore, a combined laparoscopic pyelolithotomy with RIRS was planned.
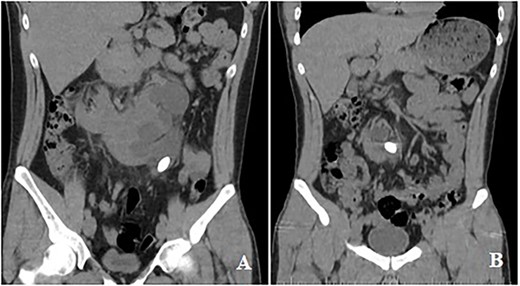
CT images: CT showed moved stone in the left renal pelvis.
The procedure was conducted under general anesthesia, with the patient in the conventional lithotomy position. Utilizing a semirigid ureterorenoscope, the renal pelvis was accessed using a guide wire, allowing visualization of the stone. The access sheet was placed into the left ureter, followed by inserting an 8-Fr Foley catheter in the patient. The catheter is attached to the access sheet. The patient was repositioned in the lateral decubitus position. Following the establishment of sterile conditions, the peritoneum was accessed laterally to the rectus muscle using a Veress needle, and abdominal insufflation with CO2 was initiated. Then, a 10-gauge trocar was inserted through the lateral umbilicus, providing visualization of the intraperitoneal region. Additional 10-gauge and 5-gauge trocars were placed. Subsequently, the Toldt line underwent dissection. An access sheet was observed in the left ureter. By carefully tracing the course of the ureter, dissection was continued until it reached the left renal pelvis. The flexible ureterorenoscopy (f-URS) was inserted through the access sheet, allowing visualization of a stone within the left kidney. As shown in Fig. 2(A and B), the pelvic wall was identified using f-URS, and the marked area of the left renal pelvis, as indicated by f-URS, was incised using laparoscopic scissors (Fig. 2C). The stone was extracted using laparoscopic forceps (Fig. 2D). A guidewire was passed through the access sheet and advanced to the incision site. Subsequently, a 4.8-Fr, 24-cm double-J (DJ) stent was placed in the renal pelvis over the guidewire. Verification of the DJ catheter placement was performed using a scope. Under scope guidance, the access sheet was removed, and a two-way, 16-Fr catheter was replaced. The renal pelvis was meticulously sutured using a continuous 3.0 Vcyril suture technique. After the bleeding was controlled, a drain was placed in the lodge. The procedure was completed.
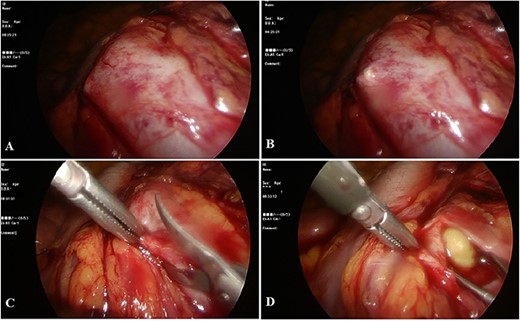
During operation: A and B: marking the location of the stone; C: opening of the renal pelvis with laparoscopic scissors; D: the process of removing stone.
Discussion
The horseshoe kidney is a prevalent congenital anomaly characterized by the fusion of the kidneys. Various morphological anomalies, including malrotation, ectopia, and vascular nutrition disorders, have been identified in the pathogenesis of the disease [3]. An estimated 40 percent of individuals are affected by the development of kidney stones due to an underlying anomaly. While it is asymptomatic in around one-third of individuals with a history of stones, the remaining individuals have complaints such as flank pain, fever and chills, and frequent urination [4]. Medical, ESWL, and surgical treatment options are available for kidney stones.
PNL is the recommended surgical treatment for kidney stones larger than 2 cm. In the case we presented, however, PNL treatment entails a risk of complications due to the horseshoe kidney anomaly and the deterioration of its existing anatomy. In addition, the applicability of PNL was considered challenging because the location of the stone had shifted during imaging. The stone was located with RIRS and removed with simultaneous laparoscopic pyelolithotomy, a procedure not previously reported in the literature. Laparoscopic pyelolithotomy combined with RIRS was successfully performed without complications for the patient. If there were any broken fragments remaining after the operation, ESWL could have been considered as a potential treatment option based on the literature on the subject. However, in our specific situation, it was not required as the stone was completely removed.
Conclusion
Our study has demonstrated that laparoscopic pyelolithotomy guided by RIRS can be a suitable treatment option in challenging conditions where kidney stone management is difficult. In healthcare institutions with enough surgical expertise, the combination of RIRS and laparoscopic pyelolithotomy provides a safe alternative to PNL options for patients with horseshoe kidney anomalies and associated kidney stones.
Conflict of interest statement
None declared.
Funding
None declared.
Data availability
Data is available upon request. Requests to access the dataset should be sent to eyupburaksancak@comu.edu.tr.

{kind=link}
{kind=link}