





Abstract
Intestinal stoma formation is an important and frequently performed procedure in emergency and elective general surgery. Parastomal evisceration is an extremely rare complication of stoma formation. The literature to date consists of a small number of case reports only. We report the case of a 54-year-old patient who presented 1-year post-loop ileostomy formation with a large parastomal evisceration. This was managed with emergency laparotomy. Our case highlights the high morbidity of this rare complication and the importance of emergent management and patient’s education.
INTRODUCTION
Parastomal evisceration is an extremely rare complication of stoma formation. The literature to date consists of a small number of case reports only [1]. This serious complication usually occurs in the early post-operative period. There are two reported cases of late parastomal evisceration 1 year or more post-operatively [2, 3]. The site of evisceration was a colostomy in both cases.
Herein, we report the case of a 54-year-old patient who presented with 1-year post-loop ileostomy formation with a large parastomal evisceration.
CASE
We report the case of a 54-year-old male who presented with a parastomal evisceration. Upon presentation, there was >100 cm of dusky small bowel eviscerated at the site of a loop ileostomy in the right iliac fossa (Fig. 1). The patient had remained at home for several hours after the evisceration occurred and was unaware of the urgent nature of the situation.
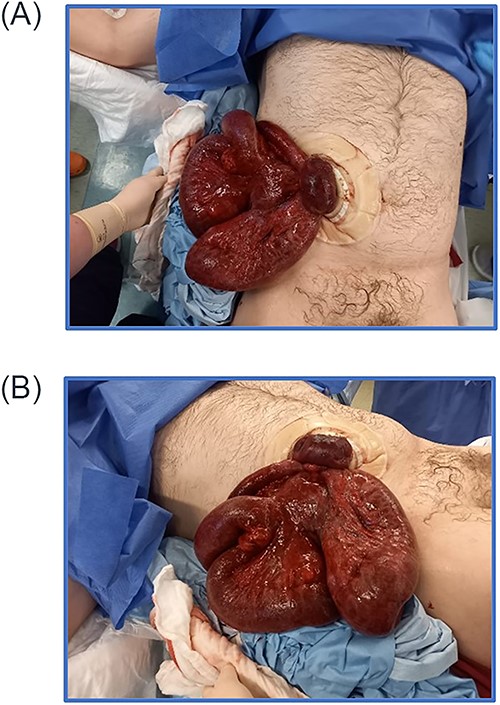
(A) Photos of eviscerated small bowel content; (B) photos of eviscerated small bowel content.
The patient’s loop ileostomy was formed 1 year prior at the time of an ileocecectomy for Crohn’s disease. The patient’s Crohn’s disease was refractory to medical management. The initial surgery was uncomplicated, and histology demonstrated active fistulating Crohn’s disease of the terminal ileum.
It was an elective surgery and the patient remained well without any medical treatment for Crohn’s post-operatively. He was seen regularly by a stoma nurse and had no active stoma issues such as high output, prolapse or otherwise. He was an ex-smoker with a 40-pack-year history.
Treatment
The patient required resuscitation for septic shock upon presentation to the emergency department. The history revealed a delay in presentation as the patient had spent several hours at home prior to seeking medical attention. The patient had not recognized the emergent nature of the issue. Following initial resuscitation, he proceeded directly to emergency surgery.
The patient underwent rapid sequence induction and was placed in a supine position, painted and draped for an emergency laparotomy. The stoma site was extended to allow the safe, immediate reduction of eviscerated content and a midline laparotomy was performed. The eviscerated contents were reduced, and the mesentery which had twisted upon evisceration was returned to its anatomical position. Despite adequate resuscitation and warming, the original stoma along with all eviscerated contents were not viable. A resection was performed, and a new end ileostomy was fashioned at a new site on the left side of the abdomen; 280 cm of healthy small bowel was measured in stepwise fashion and was confirmed proximally from duodenojejunal flexure to the new stoma.
He was treated for a lower respiratory tract infection in the immediate post-operative period which was identified on early X-ray. An organizing pneumonia with mucous plugging was confirmed with computerized tomography imaging. The respiratory tract infection was treated with intravenous antibiotics. He was discharged on Day 18 post-operatively. A surgical site infection at the site of evisceration was managed with wick dressings (Fig. 2).

Post-operative wounds and new end ileostomy.
Post-operative histology demonstrated non-viable small bowel of 110 cm, with viable margins. There was evidence of serosal inflammation and bowel wall congestion consistent with ischaemic changes (Fig. 3). There was no evidence of active Crohn’s disease.
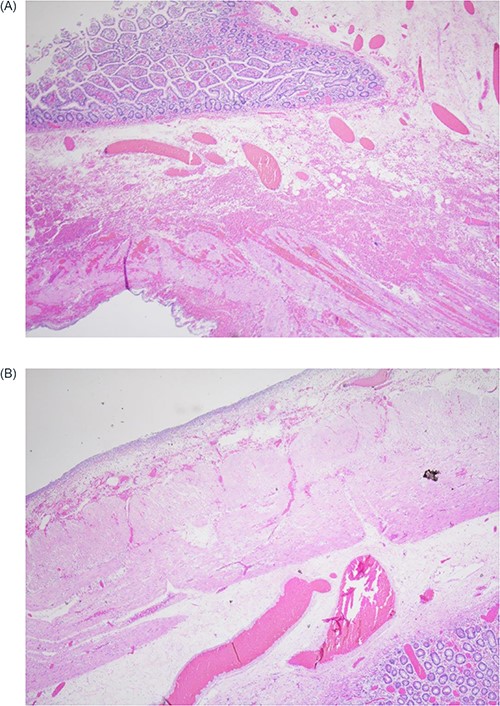
(A) Histology image demonstrating marked congestion, thinning and ischaemic change of bowel wall; (B) histology image demonstrating serosal inflammation consistent with perforation.
DISCUSSION
Intestinal stoma formation is an important and frequently performed procedure both in the emergency and elective general surgeries. It can be used in the management of benign and malignant intra-abdominal pathology. While there are commonly recognized complications including herniation, prolapse, stenosis, retraction and ischaemia, there is little research in parastomal evisceration [4]. This is an extremely rare but highly morbid complication of intestinal stoma formation. In the small number of case reports in the literature, it occurs in the early post-operative period. For our patient, this abdominal catastrophe occurred >1 year following their initial surgery.
There is not enough evidence to date to confirm the confounding and precipitating factors of parastomal evisceration. However, in our case report, we note that the patient had evidence of an evolving pneumonia and a strong pack-year history. Any cough in the preceding days would cause increased intrabdominal pressure [5]. This is a potential predisposing factor which is also highlighted in other case reports to date [1]. We also consider the patients history of fistulating Crohn’s disease in the terminal ileum but recognize no evidence of an active Crohn’s disease at the time of emergency surgery.
The benefits of patient’s education around stoma formation are well recognized [6]. It can significantly reduce hospital costs, length of stay and improve the psychosocial outcomes for patients. While parastomal evisceration is an extremely rare complication of stoma formation, patient’s education on general stomal complications and the need for urgent surgical review is important in stoma therapy. Presentation was delayed in our case as the patient was unaware of the urgent nature of his complication. Once the patient had observed evisceration at his stoma site, he rested at home aiming for self-resolution of this new finding. As a result, there was a significant delay between evisceration of his abdominal contents and seeking medical attention. In addition, the patient was profoundly shocked consistent with septic shock at presentation requiring intensive resuscitation. The histology of resected bowel demonstrated ischaemic changes without active Crohn’s disease. This was a time-sensitive pathology, and ultimately, the patient lost a significant amount of small bowel because of bowel ischaemia. This case demonstrates the high morbidity and time-sensitive nature of this rare complication.
Intestinal stoma formation is a common, straightforward surgical procedure but carries a small but significant risk of this highly morbid complication. Our case reiterates the importance of emergent surgical intervention to preserve the intestinal integrity to prevent such complications as intestinal failure, high output stomas and even death. It highlights patient’s education as a potential tool to combat the delayed presentation of time-critical surgical pathologies.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
No funding was received for this case report.
PATIENT CONSENT
Informed written consent was obtained from the patient and every effort was made to ensure anonymity of the patient.

{kind=link}
{kind=link}
{kind=link}