





Abstract
A neurofibroma not associated with neurofibromatosis type 1 is termed solitary neurofibroma. A solitary giant neurofibroma of the thigh is an extremely rare tumor. A 44-year-old woman presented to us with a well-defined swelling on her left thigh for 10 years. On the basis of magnetic resonance image finding, we diagnosed the tumor as a neurofibroma. We excised the tumor and the pathological findings established the diagnosis of neurofibroma. There was no recurrence 8-months after surgery.
INTRODUCTION
Neurofibromas are benign nerve sheath tumors of the peripheral nervous system. They are extremely infrequent, accounting for only 5% of all benign soft tissue tumors and may manifest as a slow-growing mass with benign clinical characteristics [1]. Neurofibromas are commonly, but not always, associated with neurofibromatosis type 1 (NF-1). Neurofibromas not associated with type NF-1 are called solitary neurofibromas and are usually <2 cm in size [2]. Neurofibromas are known to occur more frequently in the head and trunk than in other parts of the body [3]. We herein report a rare case of a giant neurofibroma of the left thigh that measured ~9.0 cm in size.
CASE REPORT
A 44-year-old woman presented to us complaining of a painless, palpable mass in her left thigh slowly growing in size for 10 years (Fig. 1). There were no other symptoms or findings during the physical examination. Physical examination revealed a mass ~9.0 cm in size that was, firm, and had a well-demarcated boundary. Her family and past medical history were unremarkable. Magnetic resonance imaging (MRI) of her left thigh, revealed a discrete, large, well-defined homogenous tumor measuring 8.0 × 3.5 cm in the anteromedial compartment of the thigh, displacing all the muscles of the medial compartment. The tumor showed an isointense signal on T1-weighted images and high-signal intensity on T2-weighted images, suggestive of myxoma (Fig. 2).
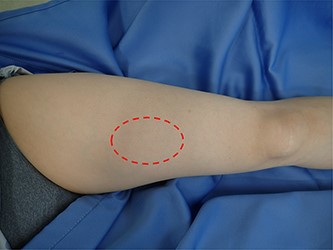
Large palpable mass in the left thigh.
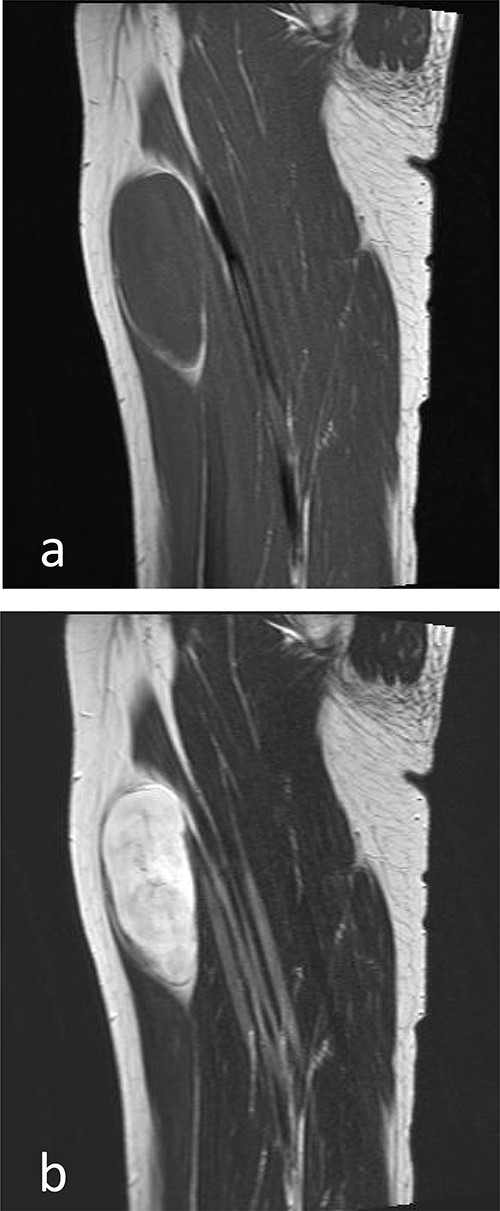
MRI imaging (sagittal section). (a) Low-signal intensity to isointense in muscles on T1-weighted images. (b) Hyperintense on T2-weighted images.
The patient underwent surgical excision of the tumor, which was identified between the rectus femoris and vastus medialis muscles. It was well capsulated and separate from the adjacent tissue. Therefore, the capsule was incised, and the tumor was completely removed. There were no adhesions to the adjacent tissue or any vascular involvement. The size of the excised specimen was 9.0 × 3.0 cm (Fig. 3).
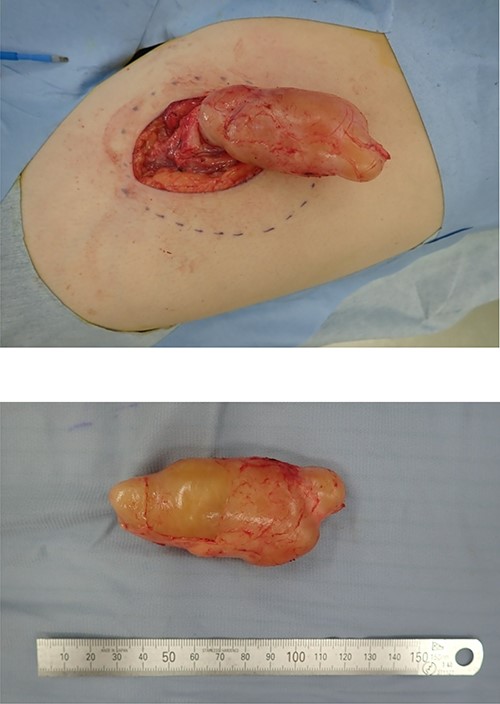
Giant encapsulated tumor after resection, ~9.0 × 3.0 cm in size. No adhesion to the adjacent tissue or vascular involvement.
Pathological examination revealed found that the tumor cells were mainly spindle cells with an abundance of a rich mucus-like substance in the background (Fig. 4). Immunohistochemical results showed positivity for CD34, a marker for muscle satellite cells, and S-100 protein, a malignancy marker (Fig. 4). These led to the diagnosis of neurofibroma. After surgery, the patient had numbness above the left knee, but no other symptoms. She experienced, no difficulty performing the activities of daily life at her 8-month follow-up, and no local recurrence was found.
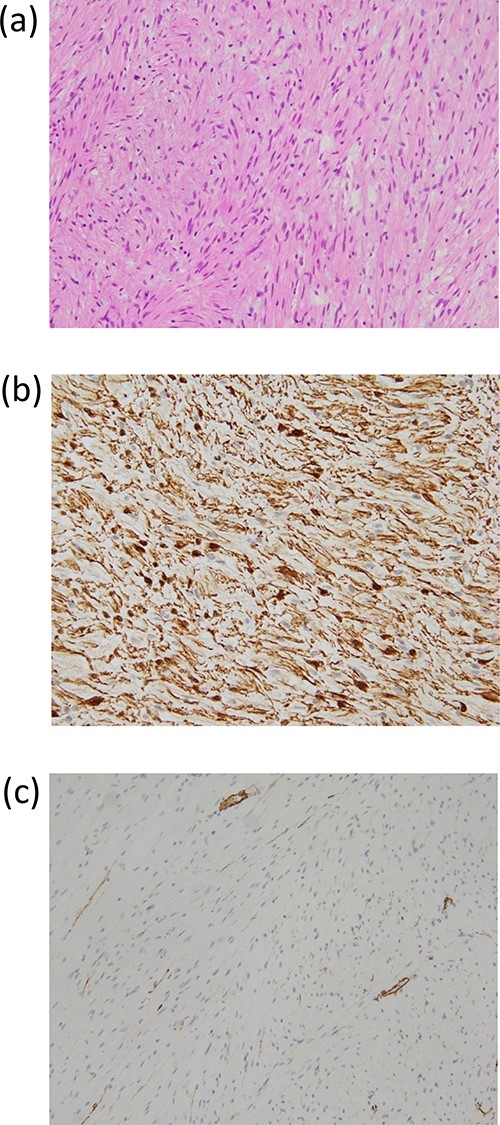
(a) Pathological findings (hematoxylin–eosin stained × 200): The tumor cells were mainly spindle cells with an abundance of rich mucus-like material in the background. Immunohistochemistry results (× 200): (b) Positive staining for S-100 protein. (c) Positive staining for CD34.
DISCUSSION
Neurofibromas are benign tumors composed of Schwann cells, perineural-like cells and fibroblasts. The age of predilection is 20–30 years, with no difference between the sexes, and they account for 5% of all benign soft-tissue tumors. Most of these tumors are solitary, but ~10% are associated with NF-1 [4]. Furthermore, neurofibromas are usually <2.0 cm in size [2] and known to occur more frequently in the head and trunk than in other parts of the body [3]. In this case, it occurred in the left thigh and was ~9.0 cm in size.
Neurofibromas associated with neurofibromatosis tend to be larger and have a higher incidence of malignancy. NF-1 can cause symptoms such as café-au-lait spots, characteristic bone lesions, focal malformations of the iris [5], but since these symptoms and family history were absent in this case. Therefore, we diagnosed the tumor as a solitary neurofibroma. This is the second case report of a giant solitary neurofibroma of left thigh.
Computed tomography showed a well-defined mass that was low-density relative to muscle and enhanced after contrast administration. Findings of neurofibromas on MRI have been reported as typically low-signal intensity to isointense in muscles on TI-weighted MR images and hyperintense on T2-weighted MR images [4, 6]. In this case, similar imaging was finding.
The final diagnosis was determined by histopathologic examination of the tumor. First, unlike schwannoma, the parent nerve of neurofibromas is typically plexiform and separable rather than solitary [7]. Second, neurofibromas are rich mucoid tissue (Antoni B area), whereas schwannomas haves a compact stroma (Antoni A area) [8]. Immunochemical analysis demonstrated positive for S-100 protein. Both neurofibromas and schwannomas are positive for S-100 protein, but only neurofibromas are positive for CD34. In the present case, immunohistochemical staining showed positivity for CD34 and thus, the diagnosis of solitary neurofibroma was made.
In summary, we have presented a case of a solitary type of giant neurofibroma of the left thigh, which is rare with regard to its size and location. The differential diagnosis of a solitary neurofibroma includes myxoid tumor, liposarcoma and schwannoma.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}