





Abstract
Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome is the second most common cause of primary amenorrhea with an incidence of 1:4000–5000 women. It is characterized by aplasia or hypoplasia of the uterus and the upper two-thirds of the vagina with normal ovaries and tubes and a normal secondary sexual characteristics. The occurrence of leiomyoma is common but it is rare to have leiomyoma in uterine remnant in MRKH syndrome. Although few cases of MRKH syndrome with leiomyoma have been reported in the literature, none presented with urinary retention. Here, we report a case of 28-year-old women who presented with urinary retention that unmasked deeply embedded huge fibroids in pelvis arising from a rudimentary uterine horns and its safe management via laparoscopic approach.
INTRODUCTION
The Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome is characterized by aplasia or hypoplasia of the uterus and vagina. Oppelt et al. [1] reported that 82% of patients have rudimentary uterine remnants. Most of the rudimentary Mullerian bulbs or remnant lack endometrial activity, and the rudimentary uteri are usually composed of smooth muscle cells, which lead to possibility of leiomyomas. It is rare to find leiomyomas in MRKH syndrome. In current case report, a woman with MRKH syndrome with deeply embedded leiomyomas presented with urinary retention. A very few cases have been reported so far, but none presented with urinary retention. Associated urinary anomalies in women with Mullerian agenesis make them more prone to urinary tract injuries and also pose difficulty in diagnosis. Proper pre-operative work up along with attention to surgical principles of lap myomectomy is the key in managing such cases.
CASE REPORT
A 28-year-old nulligravida presented to the emergency with urinary retention and abdominal pain for 2 days. She had primary amenorrhea for which workup was done at age of 16 years and diagnosis of MRKH syndrome was made. She got married at age of 20 years and was sexually active since then. She was catheterized in emergency and 2 liters of urine was drained. On examination huge abdomino-pelvic mass of around 20 weeks, nodular, hard in consistency could be palpated. Vaginal length was 7 cm with no history of sexual dissatisfaction or vaginoplasty. Magnetic resonance imaging (MRI) suggested multiple leiomyomas arising for both uterine rudimentary horns (Fig. 1). lntra-operatively, 10 × 9 × 8 cm bilobed hard myoma arising from right uterine horn with one of the lobe deeply embedded in lateral pelvic wall seen and left uterine horn seen to be harboring multiple small fibroids. Both tubes and ovaries were normal. Leiomyoma was removed by traction and countertraction and keeping ureters under vision (Fig. 2A–C). Bilateral rudimentary uterine horns along with median raphe were excised and removed to prevent recurrence (Fig. 2D and E). Post-operative period was uneventful. Histopathology report was suggestive of leiomyoma and rudimentary uterine tissue.

MRI image showing leiomyoma.
DISCUSSION
Association of MRKH and fibroids coexistence is rare, but is still a possibility. Less than 30 cases are reported in literature till date [2]. Previously reported cases aged between 20 and 66 years. Since index of suspicion for leiomyoms in MRKH is very low, diagnosis often gets missed. One case in literature presented as acute pain abdomen due to twisted leiomyoma as intra-operative finding while most of the other cases presented as lump abdomen or chronic pain. One patient presented with abdominal swelling with nocturia but none presented with urinary retention. Imaging helped clinching the diagnosis. Our case had multiple fibroids in both the rudimentary uterine horns and one of the fibroids was deeply embedding the pelvis. Most of the cases reported in literature are managed by laparotomy. Only four cases have been managed laparoscopically. We managed our case laparoscopically.
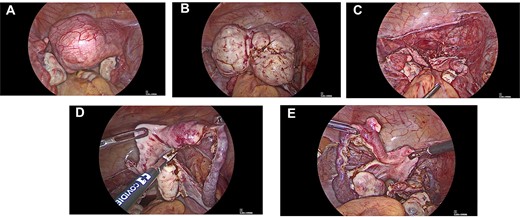
(A) Intra-operative images showing leiomyoma arising from right uterine horn. (B) Intra-operative images showing myoma dissected out of lateral pelvic wall. (C) Intra-operative images showing Mullerian buds after removal of myoma. (D) Intra-operative images showing removal of right uterine bud. (E) Intra-operative images showing small myoma in connective tissue between fallopian tube and uterine horn.
Emphasis should be on complete work up as 35% MRKH syndrome patients have associated renal anomalies [1]. Pelvic kidney should always be kept in one of the differential diagnosis in MRKH syndrome patient with a pelvic lump.
Hoo et al. [3] reported a case of 45 year old female with known MRKH syndrome with an abdominal lump. Exploratory laparotomy showed torsion of right adnexal mass and rudimentary uterus with fibroid. Removal of right adnexal mass and rudimentary uterus was done with preservation of left ovary. Histopathological examination confirmed uterine adenomyosis and leiomyoma.
A case report [4] published in 2017, presented 35-year-old nulliparous female with primary amenorrhea and 18 weeks lump in lower abdomen since 1 year. Imaging revealed multiple fibroids for which total abdominal hysterectomy was performed. Histopathology report confirmed the diagnosis.
Singh et al. [5] presented a case of a 39-year-old woman, known case of MRKH with pain abdomen, loss of appetite and weight. A provisional diagnosis of left ovarian neoplasm was made on ultrasound and computed tomography scan for which an exploratory laparotomy was performed. Finally, it was diagnosed as a case of multiple leiomyomas with hyaline degeneration.
A 50-year-old woman with a known MRKH presented with abdominal pain not responding to analgesic therapy. Due to huge size and hard consistency as well as the uncertain histologic nature of the mass, laparoscopic route was changed to laparotomy. A twisted gynecological pelvic mass was diagnosed. Histologically, the mass was described as a leiomyoma [2].
In our case, laparoscopic approach to management of huge fibroid arising from rudimentary horn and several key strategies used to minimize blood loss and injuries were:
Pre-operative delineation of course of ureters to avoid injury during surgery
Dissection of lateral pelvic side-walls to identify ureters
Fibroid removal by traction and counter-traction and care to remain inside the capsule
Complete removal of other uterine horns and the median raphe to prevent the recurrence
CONCLUSION
Although rare, possibility of leiomyoma in MRKH syndrome should be kept in mind. Clinching correct diagnosis helps in timely intervention. Complete removal of leiomyoma along with rudimentary horns should be achieved with aim to prevent its recurrence.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}