





Abstract
Obtaining durable coverage of the elbow may be challenging when surrounding tissue as well as standard free flap donor sites are not available for use. Here we describe the application of the radial recurrent artery perforator propeller flap to good effect for the coverage of the elbow joint and ulnar nerve in the context of an extensive flame burn injury of over 80% of the body surface area. Despite few descriptions of its use in the literature, it is a relatively straightforward flap to elevate and inset, the donor area was effectively autografted and there were no postoperative complications.
INTRODUCTION
The radial recurrent artery flap was first described in 1986 by Maruyama and Takeuchi as the ‘Reverse Upper Arm Flap’ [1]. Figure 1 illustrates the relevant anatomy. The artery takes origin in most cases from the radial artery or just proximal to the bifurcation of the brachial artery, below the elbow. As it ascends, it supplies supinator and the elbow, and passes between the superficial and deep branches of the radial nerve and behind brachioradialis, before lying in the lateral intermuscular septum between triceps and brachialis. It terminates by anastomosing with the radial collateral artery, one of two terminal branches of the profunda brachii artery. There are relatively few reports of this flap in the literature, especially in the context of burn injury [2–5].
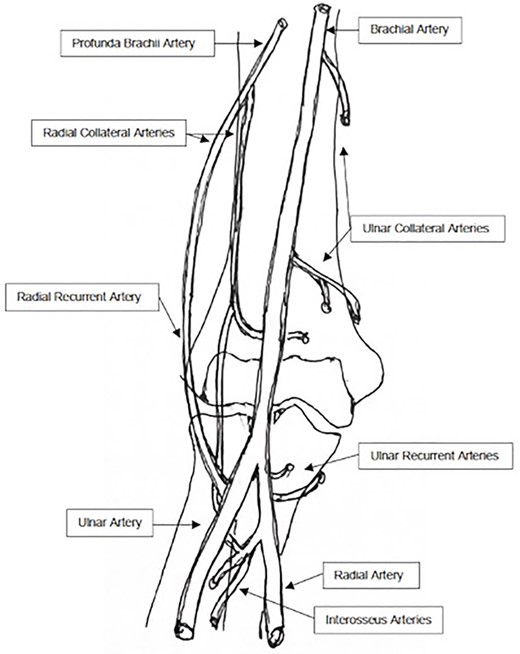
Vascular anatomy of the elbow region.
CASE REPORT
A 26-year-old female patient sustained an 82% flame burn with a grade three inhalation injury. She had a prolonged and complicated hospital course, requiring coverage of much of her body surface with a dermal substitute and meek micrografting. A radial recurrent artery (RRA) perforator flap was applied to a 30 cm2 defect of her right elbow with exposure of the joint and ulnar nerve.
The flap was marked preoperatively and perforators were identified with Doppler along the axis of the septum (Fig. 2). Under general anaesthesia and tourniquet control, we made our posterior incision onto triceps facia. This was elevated to the septum between triceps and brachialis (Fig. 3). We then turned our attention to elevating the flap to include the fascia overlying the brachialis volarly. The proximal aspect of the flap was then raised, exposing the pedicle, which was confirmed using a pencil Doppler before it was ligated (Fig. 4). We then progressed distally, dividing small branches to the triceps and protecting the radial nerve.

The debrided right elbow wound, with ulnar nerve protected, the proposed flap and axis marked based on unburned skin of the arm.
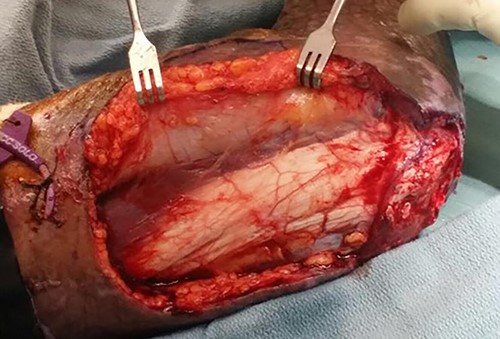
Posterior to anterior elevation towards the intermuscular septum between triceps and brachialis.
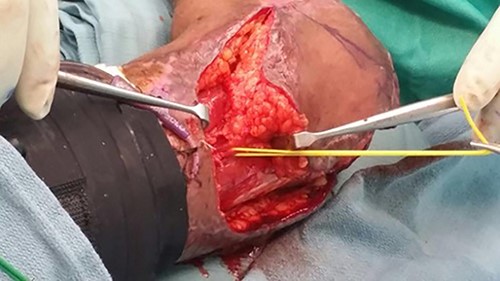
The radial recurrent artery identified and elevated with the flap and the associated fascia.
The flap was completely islanded and transposed 120° into the defect and secured without tension with sutures in two layers. A thin split skin graft was harvested and used to cover the flap donor site (Fig. 5). All areas healed well and the patient was transferred to our rehabilitation centre 2 weeks later, after which was evaluated regularly (Fig. 6). There were no short- or long-term complications of the flap, and it was re-elevated a year later to address heterotopic ossification of the elbow.

The flap inset and secured without tension, and the donor site covered with a split skin graft.

Postoperative outcome at 1 month.
DISCUSSION
Local options for coverage of the elbow are limited, with free flaps and multi-staged pedicled options often higher on the reconstructive ladder than other areas of the body. We describe a case of an extensive burn injury where much of the body was deeply burned, and most areas were therefore either skin grafted or had been used as donor sites at least once. A small area adjacent to the elbow was available, which prompted the use of propeller design of the radial recurrent artery flap was utilized. There are few reports of this flap in the literature [1–4], and none that we are aware of that utilized the propeller design in the context of a major burn injury. Propeller perforator flaps are islanded and their single artery and vein are carefully skeletonized to enable the flap to be turned up to 180° to fill a defect [6].
The radial recurrent artery flap is a reliable solution for elbow coverage in the context of elbow exposure in major burns, especially in the absence of other local or regional flap options. It possesses a consistent axial pedicle, and is relatively straightforward to elevate and inset in one stage.
CONFLICT OF INTEREST STATEMENT
None declared. Consent was obtained to display unidentifiable patient photographs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}