





Abstract
Pancreatic cancer typically presents with a cholestatic picture of jaundice, bloating and bowel changes, secondary to the obstruction of the biliary system. In tail of pancreas metastases, this clinical presentation may be absent, meaning that the disease progression can be more insidious. Cutaneous spread in pancreatic malignancies is often iatrogenic due to direct spread from the tumour site during diagnostic sampling or surgery. Rarely, cutaneous spread can be noted at distant sites, which is associated with widespread disease dissemination and poor prognostic outcomes. Our case focusses on a patient who developed metastatic spread to the chin, as a first presentation, with no other significant associated symptoms identified.
INTRODUCTION
Cutaneous spread from pancreatic malignancy is rare, commonly metastasising to the liver, peritoneum and lungs. However, a recent review has highlighted the various rare manifestations of cutaneous metastases [1]. Most common of these cutaneous spreads are the peri-umbilical lesion, such as the Sister Mary Joseph Nodule, although non-umbilical cutaneous spread has also been reported throughout the body. The latter are significantly less common and are associated with advanced disseminated disease with poor prognostic outcomes [2]. Other examples of cutaneous spread include seeding directly from the pancreas during surgery or diagnostic sampling [2]. Our report focuses on a patient who presented with a single chin lesion, which was found to be the first significant finding noted for a patient with widespread metastatic visceral spread.
CASE REPORT
Our case report describes a gentleman in his 60s who initially presented to the ENT outpatient cancer clinic at a district general hospital with a 6-week history of a lesion on his chin. This lesion gradually enlarged into a 2 × 2-cm node with central erosive changes, bleeding on contact and surface crusting. No pain was noted at any point, nor was any weight loss or change in appetite, and the patient’s only other symptoms were that of slight abdominal bloating and post-prandial dyspepsia. He had a past medical history of pre-diabetes, hypertension and a known history of chronic alcohol excess. No smoking history was noted. Family history only included lung cancer in his father and paternal grandfather.
Post-review, he was listed for an urgent biopsy under local anaesthetic. Histology showed well-to-moderately differentiated adenocarcinoma, with the likely primary being upper gastrointestinal or pancreatic in origin. Positive immunostaining was noted for CK7 and negative for p63, TTF-1, Napsin, CK20 and PSA. Magnetic resonance imaging (MRI) of the face and neck showed a 2.6-cm lesion on the chin invading subcutaneous tissues, with no mandibular involvement (Fig. 1). Due to the nature of the histology results, he underwent a positron emission tomography(PET)-computed tomography (CT) scan, which showed a cystic area in the pancreatic tail, alluding to a pancreatic adenocarcinoma primary. Widespread metastases noted included multifocal liver metastases, peritoneal lymph node, muscle and bony involvement (Figs 2–4).
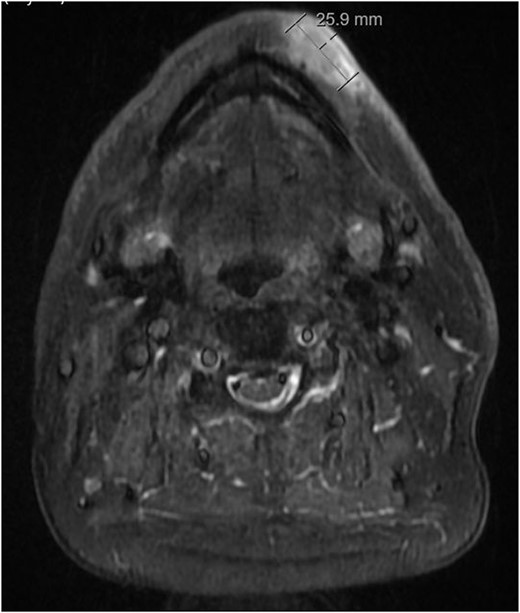
Axial STIR MRI image of lesion at level of chin.
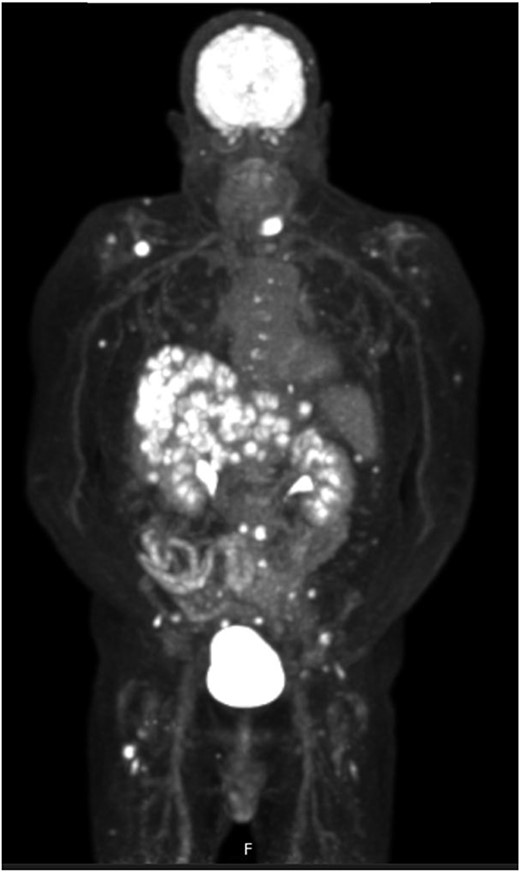
FDG PET CT imaging showing locations of metastases.
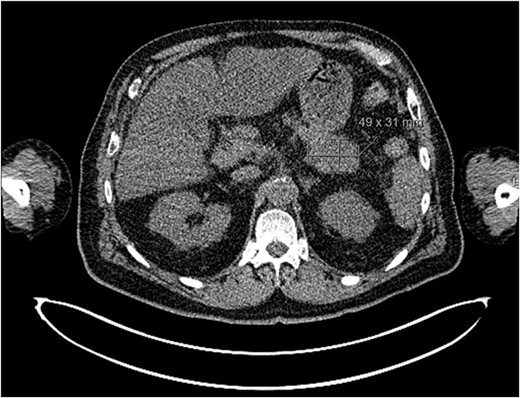
Axial CT imaging showing malignant primary at pancreatic tail.
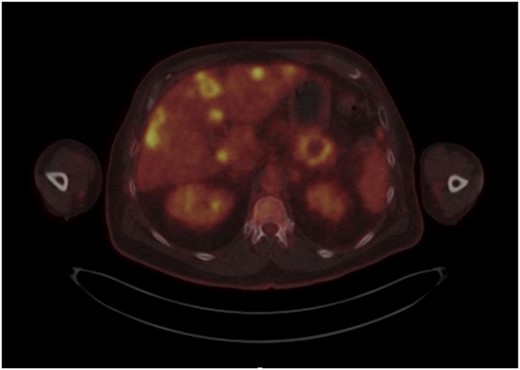
Axial FDG PET CT showing liver metasteses.
Subsequent discussion at the Hepatobilliary multidisciplinary team meeting suggested palliative, non-curative chemotherapy due to the widespread metastatic disease. Four cycles of chemotherapy were commenced 8 weeks after initial presentation, on a regime of Gemcitabine and Abraxane.
Subsequent repeat CT imaging showed initial response to chemotherapy, but our patient unfortunately passed away 4 months after his original consultation with neutropenic sepsis.
DISCUSSION
Our case is an interesting initial presentation of pancreatic adenocarcinoma that has scarcely been noted in the reported literature. With the absence of any capsule, the metastatic spread of pancreatic adenocarcinoma can occur early in the disease process through the retroperitoneal space before metastasising to the liver, peritoneum and regional lymph nodes. Cutaneous metastases in pancreatic cancer are rare and usually presents as a peri-umbilical lesion. Non-umbilical lesions are rarer still, with no definite mechanism for distant cutaneous spread identified. As of 2017, only 14 cases of pancreatic metastases to the cutaneous surface of the head have been reported, with our case showing a facial metastasis to be the initial presenting complain in already advanced disease [3]. Due to the primary being situated in the pancreatic tail, our patient understandably presented late, with the characteristic symptoms secondary to biliary obstructing absent. As such, this case illustrates a unique presentation of the upper gastrointestinal malignancies in the head and neck region.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY
The authors confirm that the data supporting the findings of this paper are available within the article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}