





Abstract
Empyema often leads to secondary thoracic deformity, but it has not been treated before. In order to eliminate the harm of this deformity, we adopted simultaneous surgery to treat empyema and secondary deformity. In this article, we introduce the operation of a 35-year-old male patient with empyema and secondary thoracic deformity. We first cleared the lesions in the thoracic cavity, and then used MatrixRIB to correct the thoracic deformity, and achieved satisfactory results.
INTRODUCTION
Empyema is an ancient and serious chest infectious disease [1–3]. In the early years, due to the lack of powerful antibiotics, the incidence of this disease was very high. With the emergence of various high-level antibiotics, this disease has been rarely seen [3]. However, in some remote areas, this disease is still not uncommon. Early empyema can be acute, if the treatment is not thorough, it can be transformed into chronic. One of the main pathological changes of chronic empyema is pleural thickening, which may cause depression of chest wall and further cause other complications, such as scoliosis [2]. Especially for the patients before puberty, empyema may result in serious secondary thoracic deformity and scoliosis. Considering the harm of these secondary lesions, it is necessary to deal with these lesions in the operation of empyema theoretically. However, no other doctors around the world have treated these lesions so far [1–3]. We found the harm of secondary thoracic deformity caused by empyema very early, so we have been performing the treatment of these lesions. This paper introduces the operation of a 35-year-old male patient with empyema. During the operation, we first cleared the lesions in the thoracic cavity, and then performed correction on the chest wall deformity, and achieved satisfactory results.
CASE REPORT
The patient is a 35-year-old male from western China. He suffered from pleuritis at the age of 17. Due to the incomplete treatment at that time, the pleuritis turned into empyema later. At the early stage, his chest wall was not deformed. From the age of 25, his right chest wall began to be depressed and scoliosis gradually appeared. During this period, he did not receive any effective treatment, and his condition gradually worsened. In half a year before admission, the patient often felt dyspnea, so he was admitted to our hospital for surgical treatment. The preoperative physical examination showed that the patient’s chest was asymmetric, the right side was largely depressed (Fig. 1A), the breath sound was low and the spine was scoliosis. Imaging examination showed that the right chest wall was depressed and shrunk, there were obvious lesions in the right thoracic cavity and the pleura was thickened (Fig. 1B and C). The patient was diagnosed as right empyema with right chest wall depression and scoliosis before operation. After full preparation, his operation was performed under general anesthesia. Left lateral decubitus position was adopted, and the right subaxillary longitudinal incision was performed. Subcutaneous and muscular tissues were dissected to expose the right ribs (Fig. 2A). After the ribs were cut in crisscross way, the thickened pleura was exposed (Fig. 2B). The pleura is stripped, and all lesions in the thoracic cavity were cleared. The thoracic cavity and surgical field were washed repeatedly, and then the chest wall was reconstructed with MatrixRIB. Firstly, the two ends of the cut rib were stretched as far as possible, and then MatrixRIB was used to extend and fix the two ends (Fig. 2C). Thoracic cavity and surgical field were washed again. After drainage tubes were retained, the incision was closed and the operation was completed (Fig. 3). There were no complications during the operation and the postoperative recovery was satisfactory. After operation, the right chest wall depression was basically eliminated, the chest wall was symmetrical on both sides and scoliosis was significantly reduced. The drainage tubes were pulled out 8 days after the operation. The incision healed well and the suture was removed 14 days after the operation. He was discharged 15 days postoperatively without any complaint.
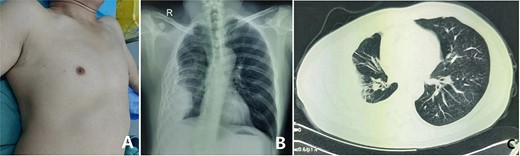
(A) Preoperative chest wall appearance; (B) X-ray examination and (C) computed tomography examination.
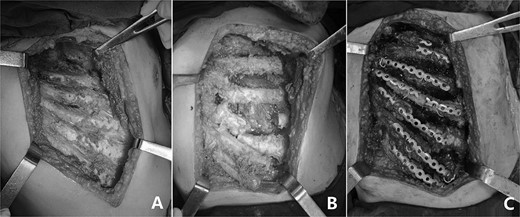
(A) The depressed ribs were exposed; (B) The ribs were cut in crisscross way and (C) The deformity was corrected with MatrixRIB.

Postoperative chest wall appearance.
DISCUSSION
The focus of empyema starts in the thoracic cavity [1–3]. If not treated in time, it may lead to secondary deformity of the chest wall [2]. After the deformity occurs, the force balance on both sides of the spine is disturbed, which may lead to scoliosis. It can be seen that empyema is a very harmful disease, and effective treatment is needed once it is found. Considering the harm of secondary deformity, it should be eliminated at the time of the operation of empyema. Scoliosis is secondary to chest wall deformity. If the deformity can be corrected in time, scoliosis will also be eliminated or alleviated. Therefore, scoliosis does not require special treatment. However, no one has ever dealt with secondary deformity before [1–3]. The causes may be related to three factors: (i) failure to recognize the importance of deformity correction; (ii) there is no proper method and (iii) concern that the use of reconstruction materials will affect wound healing.
Our department is an independent chest wall surgery department, and various chest wall diseases are the objects of our treatment [4–6]. In our patients, chest wall deformities accounts for the majority, among which there are also some secondary deformities. The treatment of these patients provides us with special vision and experience, and also lays a foundation for the treatment of empyema patients with secondary deformity. In our surgery, we use MatrixRIB to lengthen and fix the ribs on the deformed chest wall, and the results turn to be very satisfactory.
MatrixRIB is a material developed for rib fracture fixation. In our work, we found that it can be used for correction of various thoracic deformities [7–10]. Because this material has good performance, we use it in the operation of secondary thoracic deformity caused by empyema. Considering that MatrixRIB is a foreign material, in order to eliminate the impact on wound healing, we repeatedly washed the surgical field and thoracic cavity during the operation, thus ensuring satisfactory wound healing. After our treatment, not only the lesions in the thoracic cavity were completely removed, but also the patient’s thoracic shape returned to normal, and scoliosis was significantly improved. Our experience shows that the operation of empyema and secondary deformity at the same time is an ideal choice for the treatment of such diseases.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
References
Wang W, Long W, Liu Y, Cai B, Luo J.
Wang W.
Wang W, Long W, Liu Y, Cai B, Luo J.
Wang W, Long W, Liu Y, Cai B, Luo J.
Wang W, Long W, Liu Y, Cai B, Luo J.

{kind=link}
{kind=link}
{kind=link}