





Abstract
Morgagni hernias are a rare form of congenital diaphragmatic hernia, commonly found on cross-sectional imaging. Repair is generally performed electively for pulmonary or gastrointestinal symptoms. Our case presented acutely with gastric obstruction. Two months prior she had a small bowel obstruction and underwent computed tomography, diagnostic laparoscopy, lysis of adhesions and takedown of the falciform ligament, where a ‘groove’ to the left of the falciform was noted, but not repaired. We collected the presentation, technique, complications and results of 12 prior cases. A trans-abdominal, robotic-assisted tissue repair of the diaphragm with mesh reinforcement utilizing as few as three ports appears to be safe and effective. The robotic platform offers additional degrees of freedom, making retrosternal operating more ergonomic to the surgeon. The rapid progression of our patient suggests that repair at the time of discovery should be considered so that the serious complications can be avoided.
INTRODUCTION
The Morgagni hernia is a retrosternal defect between the sternum and costal attachments of the diaphragm first described in 1769. The defect is congenital and present during childhood, but diagnosed later in life after pulmonary, gastrointestinal or nonspecific thoracoabdominal symptoms such as pressure or pain. Pulmonary symptoms can include shortness of breath or recurrent pneumonia infections. Gastrointestinal symptoms can include gastroesophageal reflux, dysphagia, regurgitation or obstruction. These symptoms generally prompt a diagnostic workup including cross-sectional imaging leading an elective repair. The rarity of the diagnosis makes it difficult to standardize recommendations for method of repair.
Open, minimally invasive and robotic-assisted repairs have been described for both trans-abdominal [1–5] and trans-thoracic approaches [6]. There is only a recent case report suggesting viability of the robotic platform being used in the setting of acute presentation [5]. We performed a literature search on the use of the robotic platform and surgical techniques to assist in making recommendations on future cases. A PubMed search was performed to find all reported adult cases of Morgagni hernia repair in using a Robotic platform (DaVinci, Intuitive, Sunnyvale, CA). We collected the presentation, approach, technique, complications and results of all reported cases, including our owncase.
CASE REPORT/SERIES
Our case involved a 72-year-old female presenting acutely with symptoms of gastric obstruction. Two months prior she had surgical treatment for a small bowel obstruction. Her management included computed tomography (CT) scan evaluation (Fig. 1, top row), diagnostic laparoscopy, lysis of adhesions and takedown of the falciform ligament. At that operation a ‘groove’ to the left of the falciform was noted and photographed (Fig. 2, top left). No repair was performed. A follow-up CT after 11 days again showed no herniation into the defect. Upon her re-presentation 2-month later with gastric obstruction, her CT showed a Morgagni hernia with an incarcerated left hepatic lobe and gastric antrum (Fig. 1, bottom row). Nasogastric decompression improved her symptoms. She was then explored using one 12 mm and two 8 mm robotic ports. She was found to have auto-reduced her stomach, but her liver required surgical reduction (Fig. 2, top right). There was no hernia sac involved in the defect (Fig. 2, bottom left). This allowed free communication between the abdomen and right chest. The defect was repaired using running 2-0 V-Loc (Medtronic, Minneapolis, MN) and interrupted 0-Ti-Cron (Medtronic, Minneapolis, MN) sutures (Fig. 2, bottom right). This was reinforced using a Parietex (Medtronic, Minneapolis, MN) coated mesh. She did well after surgery and was discharged postoperative Day 1.
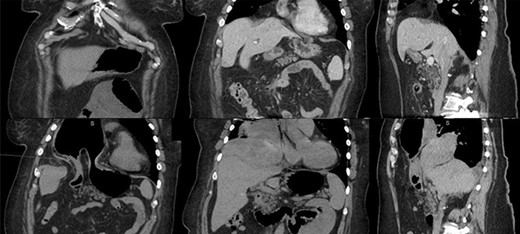
Top row: prior admission imaging. Top left: anterior coronal image showing immediate retrosternal diaphragmatic defect. Top middle: posterior coronal image showing liver abutting diaphragmatic defect. Top right: sagittal image showing liver covering diaphragmatic defect. Bottom row: imaging at time of acute incarceration. Bottom left: anterior coronal image showing incarcerated gastric antrum. Bottom middle: posterior coronal image showing incarcerated left hepatic lobe. Bottom right: sagittal right paramedian cut showing incarcerated liver and stomach.
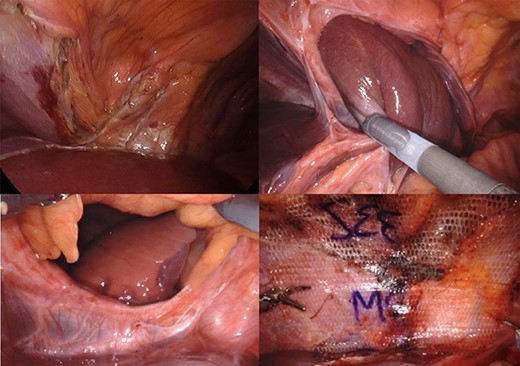
Top left: imaging from prior diagnostic laparoscopy, after lysis of the falciform ligament. Top right: image from re-presentation during reduction of left lobe of liver. Bottom left: patent foramen of Morgagni with no hernia sac showing right lung and pleural space. Bottom right: repair of hernia using 2-0 V-Loc, 0 Ti-Cron and Parietexmesh.
Our search found 13 prior adult cases of Morgagni hernia repair using the robotic platform. Patients’ ages ranged from 21 to 78 years. Nine prior cases in the literature were all performed electively for a combination of pulmonary and foregut symptoms, with only one recent abstract reporting the use of the robot in the acute setting. Including our case, 13 cases were performed via a trans-abdominal approach; one was performed via a trans-thoracic approach due to lack of a definitive preoperative diagnosis. Trans-abdominal repairs utilized three to five ports, with fewer ports required later in the series by Wei et al. and our current case. Most cases are right sided and include herniated stomach, omentum and/or transverse colon. Where described in prior reports, the trans-abdominal repairs were reinforced with a mesh. There was no standard mesh used; seven cases used composite meshes, three cases’ mesh were not listed, two used bioabsorbable and one used a biologic mesh. Cases lasted two to four hours of operative time. There were no significant reported complication and patients were discharged with 4 days, usually postoperative Days 1 or 2.
DISCUSSION
The accumulation of 13 robotic-assisted trans-abdominal repairs of Morgagni hernias suggests increasing viability and safety of the platform. Apposition of the diaphragm to the retrosternal tissues with mesh reinforcement has been standard in all described cases. The robotic platform offers additional degrees of freedom making retrosternal operating more ergonomic to the surgeon. It appears experience on the platform and with prior cases can decrease the operative time and the number of ports needed. Two recent cases have shown the viability of the platform in emergency general surgery. In our case, the rapid evolution from an asymptomatic to acutely symptomatic hernia involving the liver and stomach suggests caution should be advised when encountering incidental small diaphragm defects. Repair at the time of discovery should be considered so that potentially serious complications associated with incarcerated viscera might be avoided.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}