





Abstract
Liposarcoma is a common occurrence over retroperitoneum. However, dedifferentiated liposarcoma is an uncommon variety affecting the small bowel mesentery, making it a rarity. We report a case of 56-year-old male presented with the lump in the abdomen. Computed tomography abdomen revealed well-defined space-occupying lesion. Laparotomy was done and mass was excised along with segment of ileum to achieve negative margin. Histopathology and immunohistochemical study helped in determining mass to be dedifferentiated liposarcoma of mesentery. Therefore, liposarcoma should be considered in differential diagnosis of abdominal mesenchymal tumors. Surgical resection to achieve negative margin is the mainstay of treatment for mesenteric liposarcomas.
INTRODUCTION
Liposarcoma is the second most common sarcoma with retroperitoneum being the common site in abdomen [1]. Liposarcoma is classified as well-differentiated, myxoid, round cell, pleomorphic and dedifferentiated by WHO [2]. Primary mesenteric dedifferentiated liposarcoma is the extreme rarity of a disease [3].
CASE REPORT
A 56-year-old male presented with pain and palpable mass in left abdomen for over a week period. His bladder and bowel habit was normal including his weight. His past medical history included hypertension. The physical examination of the abdomen revealed mobile, hard mass over left lower quadrant of the abdomen.
Laboratory test including tumor marker (carcinoembryonic antigen) was normal. Abdominal ultrasonography revealed heteroechoic mass over left iliac fossa with regular borders. Computed tomography (CT) of the abdomen revealed well-defined space-occupying lesion of size 10 × 8.5 × 7 cm at the left iliac fossa. There were no areas of calcification; however, plane between the mass and the bowel was lost in few places suggesting of invasion (Figs 1 and 2).

CT abdomen showing mass in coronal cut.
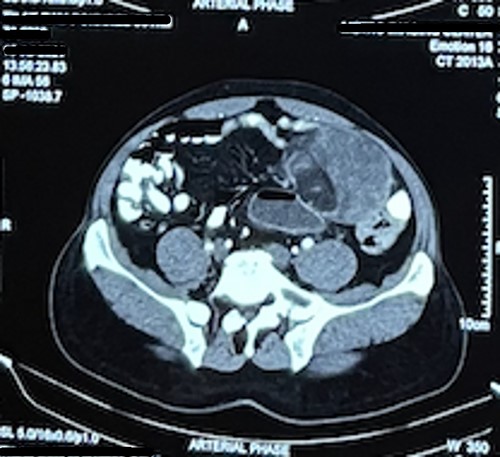
CT abdomen image of the mass in the transverse cut.
Patient was admitted. Midline laparotomy was done. Peritoneal cavity was explored. Large lipomatous mass measuring 13 cm × 8 cm was found at ileal mesentery at ~70 cm from ileocecal junction. Mass was well defined with invasion into the bowel and the ileal arteries. Mass was excised in toto along with involved ileum attaining macroscopically negative margins. Bowel continuity was maintained with end-to-end anastomosis (Fig. 3). Postoperative period was uneventful.

Resected mass along with the mesentery and ileum.
Gross examination revealed large lobulated mass of size 12 cm × 10 cm × 7 cm, weighing 817 g. The cut section showed yellow soft to firm areas with some hemorrhagic areas. Eosin and hematoxylin stain revealed area of lipoblast, pleomorphic cell, mitotic figures with multiple areas of necrosis (Figs 4, 5 and 6). Immunohistochemical reaction showed positivity for S-100 protein, mouse double minute 2 (MDM-2), cyclin-dependent kinase 4 (CDK4) and p16 which helped us differentiate it as dedifferentiated liposarcoma.
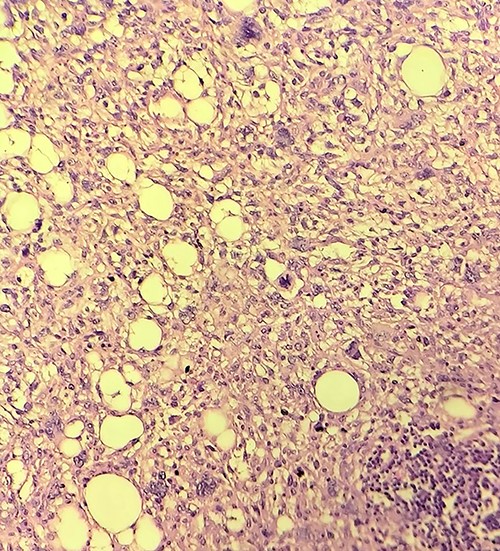
Histopathology of the mass.
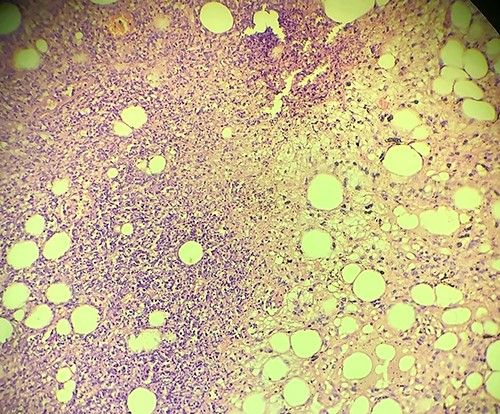
Histopathology of the mass showing area of necrosis.
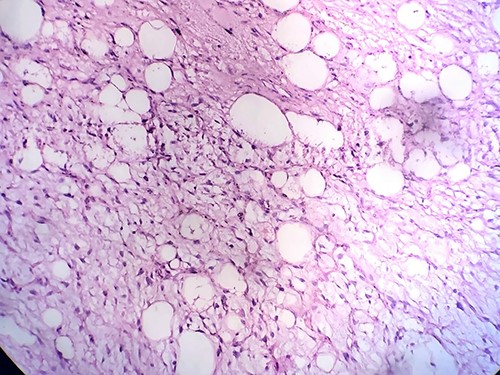
Histopathology of the mass.
DISCUSSION
Liposarcoma is the second most common sarcoma; however, primary mesenteric liposarcoma is extremely rare. Less than 50 cases have been reported so far, even fewer being the dedifferentiated type [4]. Evan [5] in 1979 first introduced dedifferentiated as a new term to describe liposarcomas containing mixture of atypical, well-differentiated and high-grade non-lipogenic sarcomas with transition between components.
Mesenteric liposarcomas is common among males of 50 and 70 years. It is locally aggressive, non-metastasizing and presents as a deep-seated mass along the root of mesentery. It can grow into a large-sized mass [4]. Patients present with nonspecific symptoms of pain in abdomen, lump in abdomen, abdominal distention and weight loss early satiety [6, 7]. CT helps in determining the size, characteristic and invasion to adjacent organs. CT images shows well-defined to poor margination, invasion, contrast enhancement, inhomogeneity and CT numbers greater than normal fat [8].
Liposarcomas are divided into myxoid, pleomorphic, well-differentiated, dedifferentiated and round cell type [1]. Myxoid variety is the commonest of the liposarcoma found in 50% of the cases [8]. Dedifferentiated liposarcoma is a pleomorphic/undifferentiated sarcoma mixed with well-differentiated liposarcomas exhibiting wide spectrum of morphology [3, 9]. Dedifferentiated liposarcoma is often detected as metastatic or recurrent lesions rather than primary lesion, which is rare as in our case [9]. Of the various immunohistochemical examinations MDM2 and CDK4 show better sensitivity and specificity of 97% and 92%, and 83% and 95%, respectively [10]. Also, S-100 helps in distinguishing liposarcomas from malignant fibrous histiocytoma [11].
Complete resection of tumor along with partial or complete resection of the involved organ is the only effective treatment option [3]. Therefore, achieving negative margin during resection is associated with disease-free survival and overall survival [12]. Major problem with the dedifferentiated liposarcoma is chance of metastasis which is 17%, local recurrence of 40% and tumor-related mortality of 28%. Hence, it requires close monitoring postoperatively [3, 9]. Role of adjuvant chemotherapy is debated and remains unclear. Radiotherapy is associated with overall survival of the patient; however, it is avoided in the cases of mesenteric liposarcoma due to risk of radiation ileitis [9, 13].
CONCLUSIONS
Primary mesenteric liposarcoma is rare; it presents as slow growing abdominal mass. Among liposarcoma dedifferentiated type has the worst prognosis and chance of recurrence so regular follow-up of patient after complete surgical resection with negative margin is required. Proper histopathological diagnosis in determining the type of liposarcoma is essential for prognosis. Role of adjuvant chemotherapy is yet to be established.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}