





Abstract
Ureterorenoscopy (URS) is a minimal invasive procedure used for diagnosis and management of the upper urinary tract. Due to the vast advancement in URS technologies, the efficacy and safety greatly improved with lower complication rates. Intussusception is a rare complication of URS. We report a case of iatrogenic ureteral intussusception that was managed with ileal interposition.
INTRODUCTION
Flexible Ureterorenoscopy (F-URS) is a minimal invasive procedure used for diagnosis and management of the upper urinary tract. Due to the vast advancement in Ureteroscopy (URS), the efficacy and safety greatly improved with lower complication rates. The overall complication rate of URS is 7.5% [1]. The complication of URS can be divided into major and minor complications. Major complications include ureteric perforation, tears, avulsion, sepsis and intussusception. Intussusception is a rare complication of URS. To the best of our knowledge, few cases were reported as iatrogenic intussusception secondary to ureteroscopy. We report the first case of iatrogenic ureteral intussusception due to Flexible URS which was managed with ileal interposition.
CASE REPORT
This is a case of 48-year-old man Hypertensive on medication who underwent bilateral percutaneous nephrolithotomy 10 years ago for bilateral renal stones. Patient was referred to our center as a case of left ureteric injury post Flexible URS for left middle and upper ureteric stones and was managed with left DJ stent. Abdominal CT scan showed stones in the left ureter with no leak (Fig. 1). Two months later, we decided to perform retrograde pyelography (RGP) and eventually ureteroscopy in order to clear his stones. RGP showed an invagination of mid-ureter about 4–5 cm (Fig. 2). A guidewire was passed under fluoroscopy guidance. Stones were removed and endoscopic exploration revealed ureteral intussusception (Fig. 3). DJ stent was inserted, and 6 weeks later, we performed a nuclear scan (MAG3) that showed obscure drainage from the left kidney. Therefore, ureteral reconstruction with ileal interposition was our option to overcome this complication. Patient underwent the surgery uneventfully and was followed up after surgery for 6 months and was pain free with no significant hydronephrosis or change in renal function.

CT scan of abdomen showing left JJ stent in place with multiple upper ureteric stones with obvious leak.
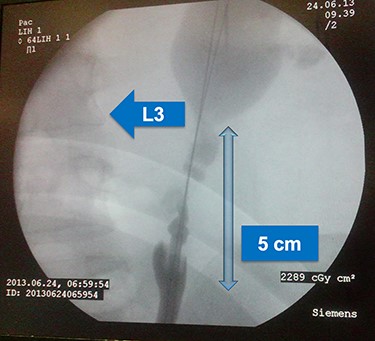
Retrograde pyelogram showing invagination of mid ureter for about 4–5 cm, lumbar vertebra 3 is shown for orientation.

Endoscopic image during ureteroscopy showing ante-grade invagination of the ureter.
DISCUSSION
Ureteral intussusception is a rare diagnosis and complication. Patients usually present with a classic triad of hematuria, colicky pain and ureteral dilation as reported by the literature [2]. The etiology of intussusception is thought to be due to tumors, iatrogenic and rarely ureteric calculus [3]. Tumors include polyps, papilloma and transitional cell carcinoma. Surgical instrumentation that leads to intussusception as reported in the literature include: ureteroscopy, percutaneous nephrostomy catheter exchange and percutaneous endopyelotomy [2, 3]. The mechanism of intussusception is telescoping of the proximal ureter (the intussuscipiens), due to a combination of peristaltic activity, urinary flow and gravity pulling a section of the ureter (the intussusceptum) distally [3].
Ureteric intussusception can be diagnosed radiographically using intravenous pyelography, RGP and CT scan with characteristic sings. These signs include ‘line sign’, ‘concentric’ also referred as ‘target sign’, ‘V-shaped’ and ‘stalk-of-corn appearance’. In patients with poor renal function or allergy to contrast, MRI is an option to diagnose intussusception and was used in a case report [2].
The management of intussusception is almost surgical with one case that was managed with hydrostatic pressure as the cause was percutaneous nephrostomy exchange with a unique retrograde intussusception [2, 3]. Ureteral intussusception might be complicated with ischemia. Therefore, prompt diagnosis and management are warranted. The surgical option of intussusception depends on the underlying condition and location of intussusception. The first reported iatrogenic ureteric intussusception was due to repetitive URS as the patient was having positive urine cytology, and he was managed successfully with Boari flap [2, 3]. In a rare case of intussusception secondary to calculus, it was managed with stone fragmentation and avoiding basket retrieval along with biopsies to rule out tumors [3]. Our case is the first reported case that was managed with ileal interposition due to the large defect. Ileal ureteric replacement remains a safe and effective surgical option for long and complex ureteric defects in the hands of skilled urologists with careful patient selection [4].
CONCLUSION
Our case represents, to our knowledge, the first case of iatrogenic ureteral intussusception secondary to URS that was managed with ileal interposition. We think that ileal interposition is a valid surgical option for ureteric intussusception, when in the hands of skilled urologists with careful patient selection.
CONFLICT OF INTEREST STATEMENT
Authors declare no conflict of interest is present.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}