





Abstract
Carcinosarcoma ex pleomorphic adenoma is an extremely rare malignant neoplasm of the salivary gland that originates from a pre-existing benign tumor. Malignant transformation of the pleomorphic adenoma is extremely rare. The management of carcinosarcoma ex pleomorphic adenoma remains challenging because of its rarity, behavioral aggressiveness and resemblance to benign pleomorphic adenoma. Herein, we present the case of a 75-year-old male resident of Saudi Arabia with a history of a swelling in the right parotid gland for more than 25 years, which grew slowly with time. He underwent surgical removal with superficial parotidectomy. Afterward, histological examination of the resected tumor revealed features of carcinosarcoma, and he was diagnosed with carcinosarcoma ex pleomorphic adenoma. He presented again with recurrence of the tumor, which was managed with total parotidectomy and a combination of radiotherapy and chemotherapy. At 12-month follow-up, the patient showed no evidence of disease recurrence or distant metastasis.
INTRODUCTION
Carcinosarcoma ex pleomorphic adenoma of the parotid gland is an extremely rare malignant neoplasm. Carcinosarcoma of the parotid gland comprises only 0.05% of all salivary tumors and 0.1% of all malignant salivary neoplasms, which represent only 1–3% of all head and neck cancers [1–3]. Carcinosarcoma commonly arises as a de novo; however, in 30% of the cases it originates from pre-existing pleomorphic adenoma [2, 4]. Furthermore, pleomorphic adenoma is relatively uncommon; its incidence rate as per national-based study is from 3.9 to 4.7 per 100 000 per year [5]. Carcinosarcoma ex pleomorphic adenoma is a very aggressive tumor, with a poor prognosis and a mean survival rate of 2.5–3.6 years [2]. For years, the primary management of this disease has been surgical excision (parotidectomy), which may be followed by radiation and chemotherapy [6]. In this case report, we present a rare case of recurrent carcinosarcoma ex pleomorphic adenoma.
CASE REPORT
A 75-year-old man residing in Saudi Arabia had been having swelling of right parotid gland, which grew slowly over more than 25 years. He did not seek any medical advice during this period. He visited a hospital, and he underwent fine needle aspiration (FNA) of the swelling, which suggested a pleomorphic adenoma (Fig. 1). Subsequently, he underwent superficial parotidectomy. Histopathology of the surgical specimen revealed a carcinosarcoma.

First presentation.
During 1.5 months, the patient was managed to be referred to a medical city in Riyadh due to the lack of cancer treatment facilities in Almadinah. During that time, the patient developed a new, rapidly progressive painful swelling of the remaining right parotid gland, which was associated with tearing of the right eye (Fig. 2). Histopathology slides submitted to our histopathology department revealed carcinosarcoma ex pleomorphic adenoma. A computed tomography (CT) scan performed with contrast for the head and neck showed features of recurrence. The patient was seen by the tumor board, combining different clinical specialties, and the case was discussed with the oncologist and radiotherapist. Subsequently, total parotidectomy followed by chemoradiotherapy was planned.

Recurrence.
Total right parotidectomy with the preservation of all facial nerve’s branches was successfully performed under general anesthesia (Fig. 3). The patient tolerated the procedure and was transferred to the recovery room in good condition. The post-operative course was uneventful. The resected tissue was sent to the pathology laboratory for histopathology testing. The patient regularly visits the clinic for early detection of tumor recurrence and distant metastasis. In addition, he visits a radioimaging clinic weekly to receive adjuvant concurrent chemoradiotherapy (CCRT).

Total right parotidectomy.
Contrast-enhanced CT head and neck demonstrated a huge, irregular, heterogeneously enhancing and solid cystic lesion, which was seen arising from the superficial lobe of the right parotid gland (Fig. 4). The lesion is collectively measuring 10 × 8.4 × 4.6 cm. There were multiple, solid enhancing nodules abutting the main lesion. There was significant surrounding fat stranding with thickening of the overlying skin.
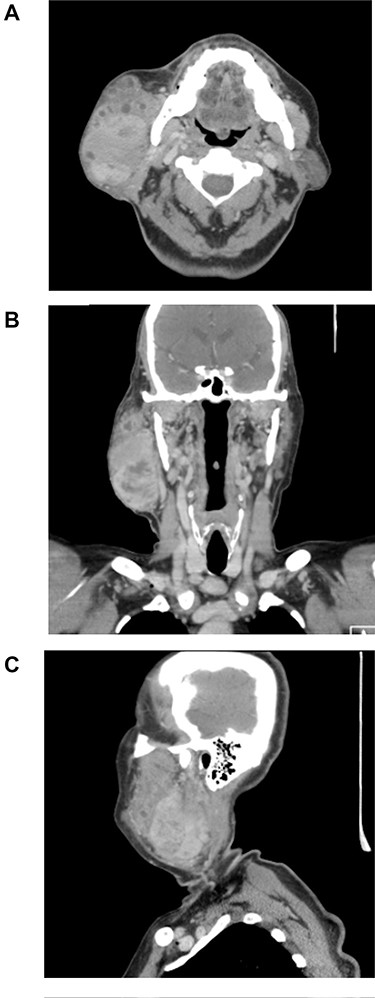
Head and neck CT on the axial (A) coronal (B) and sagittal (C) planes.
Histopathology revealed an epithelial-rich pleomorphic adenoma with frequent foci of squamous differentiation. Frequent foci of infiltrative squamous cell carcinoma (carcinoma component) were noted admixed with a large malignant chondroid matrix (chondrosarcoma component). The overall histological features were consistent with carcinosarcoma ex pleomorphic adenoma.
DISCUSSION
Features
Pleomorphic adenoma is the most common benign tumor, accounting for more than half of the salivary gland benign adenoma [7, 8]. Pleomorphic adenoma has the potential for malignant transformation. The rate of the malignant transformation is only ~3–4%, and it is directly proportional to the duration of tumor existence; the risk in the first 5 years is ~1.5%, whereas the risk is 9.5% for 15 years [3]. The risk of malignant transformation has also been linked to other factors, such as tumor recurrence, radiation exposure, tumor size and advanced age [3]. It is mostly a firm mass, and the parotid gland is the most common site of origin (60% or more), followed by the submandibular glands and the accessory salivary glands [9, 10]. Carcinosarcoma ex pleomorphic adenoma has an aggressive behavior, and the patient usually presents with a history of a long-standing, slowly growing tumor with an average of duration 10–15 years, subsequently presenting with a sudden and rapid enlargement [7]. The second most common symptom is pain. Facial nerve paresis is not uncommon, and it presents in ~14% of the patients [7].
Diagnosis
Carcinosarcoma by definition consists of two components: carcinomatous and sarcomatous components. Each of these types has its own histological types. Adenocarcinoma and undifferentiated carcinoma are the most common histological types of carcinoma, followed by squamous cell carcinoma. On the other hand, the most common types of sarcoma are chondrosarcoma and osteosarcoma, followed by fibrosarcoma, leiomyosarcoma, liposarcoma and rhabdomyosarcoma [2–4]. Due to the difficulty in differentiating between benign and malignant tumors, the definitive diagnosis is only reached through histopathological examination. For initial management, preoperative diagnosis can be established through clinical history, examination, FNA cytological findings and imaging results.
Management
The management of carcinosarcoma ex pleomorphic adenoma remains challenging due to its rarity, resemblance to benign tumor and aggressive nature. Surgery (parotidectomy) is widely accepted as the primary treatment, which may be followed by radiotherapy and chemotherapy [6]. Moreover, Bernier et al. reported 334 patients, with head and neck squamous cell carcinoma, who were randomly assigned into two groups: one received radiotherapy alone, and the other received the same radiotherapy regimen that was combined with 100 mg of cisplatin [11]. They concluded that the combination of both chemotherapy and radiotherapy is more effective than radiotherapy alone in treating those patients post-operatively. Furthermore, the rates of local and regional control of the disease, progression-free survival and overall survival were significantly higher in the combined therapy group [11].
CONCLUSION
To the best of our knowledge, this is the first reported case of carcinosarcoma ex pleomorphic adenoma in Saudi Arabia. In conclusion, although this malignant lesion mostly arises as a de novo tumor, clinicians should have a low threshold of suspicion for the possibility of such neoplasms when encountering a patient with a long-standing benign salivary gland lesion. The management of this disease should involve a multidisciplinary team to reach the optimal prognostic goal for each patient.
DECLARATION OF FIGURES' AUTHENTICITY
All figures submitted have been created by the authors who confirm that the images are original with no duplication and have not been previously published in whole or in part.
ACKNOWLEDGEMENTS
We would like to thank Editage (www.editage.com) for English language editing.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

{kind=link}
{kind=link}
{kind=link}
{kind=link}