





Abstract
We describe a case of mild lower urinary tract symptoms and microscopic hematuria in a 53-year-old-male with hypertension found to have urethral stricture disease suspicious for urothelial carcinoma. During the investigation, cystoscopy and biopsy demonstrated eosinophilic amyloid proteins consistent with primary localized urethral amyloidosis. No systemic evidence of amyloidosis was demonstrated. Following a trial of conservative management with serial dilatations, the patient elected to proceed with surgical management by anterior urethroplasty using an excision and primary anastomosis technique. The patient has done well with resolution of his symptoms and no further recurrence of urethral amyloid disease at ongoing follow up.
INTRODUCTION
Amyloidosis presenting as an isolated entity contained within the genitourinary tract is a rare occurrence with few cases reported in the literature [1–3]. The disease is characterized by eosinophilic amyloid proteins that demonstrate apple-green birefringence under a polarized light microscope following Congo red straining [2]. The condition may be localized or systemic and when presenting as the former, it often mimics that of urothelial carcinoma and thorough investigation is prompted [4].
CASE REPORT
A 53-year-old male presented with a 3-year history of slowly progressive mild to moderately severe lower urinary tract symptoms including nocturia of two to three times per night and a slow urinary stream. Urinalysis confirmed microscopic hematuria of 3–5 RBC/hpf. No history of lichen sclerosis, sexually transmitted infection, pelvic radiation, genitourinary trauma or family history of genitourinary malignancy was identified.
The patient underwent further evaluation with imaging including renal ultrasound, which was normal. Flexible cystourethroscopy demonstrated a circumferential urethral mass concerning for urothelial carcinoma (Fig. 1), which was biopsied with histopathology negative for urothelial carcinoma but positive for amyloid protein deposition. Examination of the external genitalia was unremarkable and there was no palpable induration along the ventral penile shaft. Systemic workup for additional manifestations of amyloidosis was negative. Imaging with retrograde urethrography (RUG) demonstrated an ~2 cm segment of urethral stenosis in the penile urethra (Fig. 2).

Endoscopic visualization of circumferential amyloid protein deposition causing urethral luminal narrowing.

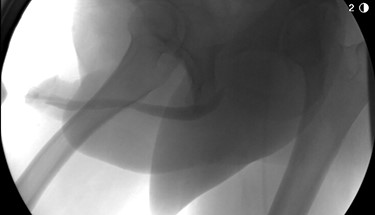
RUG demonstrating focal urethral stenosis of the penile urethra during preoperative investigation.
Given the mild nature of his symptoms, the patient initially refused surgical intervention and had been managed with intermittent urethral stricture dilatation. Eventually, the patient elected to proceed with definitive surgical management. He underwent anterior urethroplasty utilizing an excision and primary anastomosis approach which was completed successfully and without complication. Final pathology of the excised diseased segment confirmed amyloidosis without evidence of malignancy. Follow up RUG demonstrated a well-healed anastomosis without leak and excellent urethral patency (Fig. 3). At the latest follow up of 6 months, the patient continues to do well and denies lower urinary tract symptoms or hematuria.
Postoperative imaging demonstrating a well-healed urethral anastomosis with excellent patency.
DISCUSSION
Amyloidosis is a variable disease and can present either systemically (80–90%) or in a localized manner (10–20%) [5]. Diagnosis of this distinction is critical as the respective prognoses vary considerably with systemic disease being associated with a poorer prognosis. As well, the disease can be characterized as being primary or secondary depending on the nature of its protein deposition and association with chronic inflammatory diseases, as is the case in secondary disease [2]. In the case of localized disease, the clinical course is invariably benign with rates of progression being slow [4].
The risk of progression of localized disease to systemic manifestations is extremely rare and few cases have been reported [6]. The management of primary systemic amyloidosis is well established and includes a combination of oral prednisone and melphalan [7]. Improved survival has been demonstrated in patients receiving further systemic therapy with chemotherapy using Vincristine, Adriamycin [doxorubicin], Dexamethasone followed by autologous peripheral blood stem cell transplantation [7, 8].
Contrary to systemic disease, the management of primary localized amyloidosis is local excision through either an open or transurethral approach [4]. Several authors have reported the successful outcome of a combined approach of local excision and urethral reconstruction with urethroplasty with satisfactory long-term outcomes [1]. Although the risk of recurrence of urethral stricture is higher with dilatation, some urologists have advocated this approach in select patients [4]. In our patient, surgical excision and reconstruction were ultimately necessary to control the disease and the patient remains well at ongoing follow up. Crook et al. [9] have recommended a follow up period of at least 2 years to monitor for recurrence, however in most instances, recurrence is rare.
Primary localized urethral amyloidosis is a rare phenomenon and often presents in a similar manner to primary urethral urothelial carcinoma. Considering malignancy along with amyloidosis in the differential diagnosis of an obstructing urethral mass is paramount as the aggressiveness of the management approach will certainly impact patient outcomes. Surgical excision and reconstruction are often required to achieve disease stability and improve patient symptoms, satisfaction and outcomes.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}