





Abstract
Testicular ectopia is an aberrant deviation of the migration of the testis from its usual path of descent into the scrotum. Of the forms of ectopic testis, the penopubic (also called pubopenile) type is one of the least common; in this case, presented as an obstructed hernia. We report a rare case of penopubic testicular ectopia with bilateral cryptorchidism in a 17-year-old boy who presented to the emergency room with right obstructed inguinal hernia. Intraoperative findings included bilateral cryptorchidism, hernia sac with right undescended testis and normal vermiform appendix, a left penopubic testis abutting the hernia sac. Both testes had separate epididymides and adequate length of vasa deferentia and were transposed into their respective hemiscrotum via an open inguinal approach. The patient had an uneventful recovery.
Penopubic testicular ectopia can present as obstructed Amyand’s hernia. Early open groin exploration with orchidopexy was satisfactory.
INTRODUCTION
Testicular ectopia is an aberrant deviation of the migration of the testis from its usual path of descent into the scrotum [1].
The major sites of ectopic testes include superficial inguinal pouch, femoral, perineal, transverse and pubopenile [2]. The pubopenile type is the least common [1, 3].
Amyand’s hernia, though uncommon, has been reported in literature [4].The finding of vermiform appendix in the sac of inguinal hernia coexisting with undescended testis and pubopenile ectopic testis is not known much in literature. We present a case of pubopenile ectopic testis in a 17-year-old boy presenting with obstructed Amyand’s hernia. This will add to the literature and highlight the need for optimum preparedness to handle any incidental contents of hernia.
CASE REPORT
A 17-year-old male patient presented to the emergency room with a day history of sudden right inguinal pain and irreducible right groin swelling that was partially reducible and discovered since birth. He had vomiting, colicky lower abdominal pain but no distension or constipation. His scrotum was empty from birth but social reasons hampered his presentation to hospital for appropriate medical care.
He was in mild painful distress, otherwise he was clinically stable. He had normal male secondary sexual characteristics for his age. There was an 8 × 10 × 12 cm firm, tender, irreducible right inguinal mass with no differential warmth. The normal circumcised penis had normal-situated urethral meatus. Both hemiscrota appeared developed but empty (Fig. 1), with no palpable testis in the left inguinal region. A diagnosis of obstructed right inguinal hernia with bilateral cryptorchidism was made. Pcv result was 38% and urinalysis was normal. Abdominal ultrasound noted a 3 cm defect in the right inguinal region through which aperistaltic bowel loops herniated. Both testes were in the right inguinal region and were normal in size, outline, echo pattern, showed normal flow on Doppler interrogation and had no focal mass lesion. The consultant surgeon worked up the patient and did emergency groin exploration.
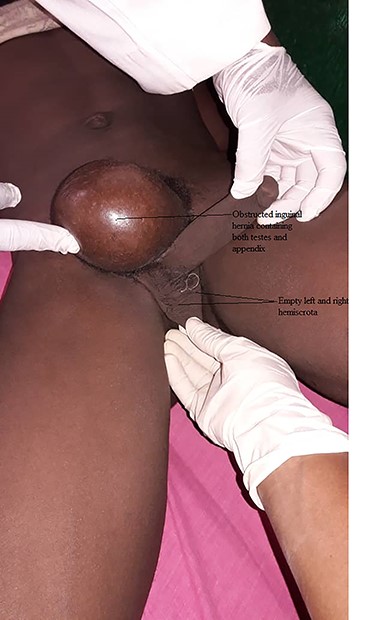
Preoperative picture showing obstructed inguinal hernia and empty scrotum.
Right inguinotomy revealed two testes of equal appearance within the inguinal region. The right testis, terminal ileum and apparently normal appendix were within the hernial sac in the inguinal canal, while the left testis was lying anterior to the sac and abutting on the right superficial ring (Fig. 2a and b). The right undescended gonad had its vas deferens and blood vessels coming from the right inguinal canal.
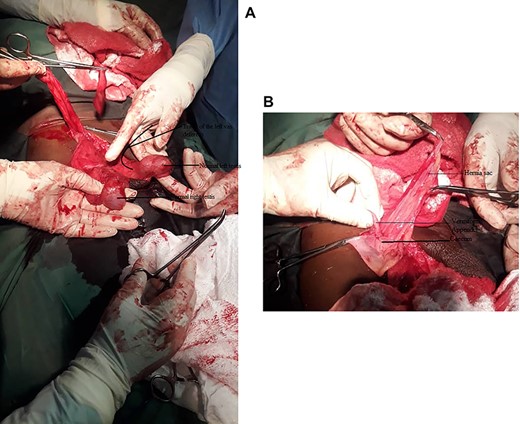
(A) Intraoperative picture showing the right and left testes. (B) Intraoperative picture showing the vermiform appendix, caecum and hernia sac.

Three months post-operative picture showing the scrotum containing both testes.
The sac was isolated and the contents were reduced and high ligation done. A left inguinotomy revealed that the vessels and vas of the left ectopic gonad originated from the left side, and passed through the left superficial inguinal ring to reach the penopubic area where it was sited. No gubernaculum was seen attached to the ectopic testes. A bilateral tissue repair of the posterior walls was performed. Both tunica vaginalis of the testes were drained of small serous fluid, excess excised and plication done. The lengths of the spermatic cords were long enough (Fig. 2) to permit bilateral orchidopexy without tension after creating dartos pouches. Convalescence was uneventful and he was discharged on the 10th post-operative day. After 3 months both testes were palpable in the scrotum (Fig. 3).
DISCUSSION
In pubopenile ectopia, the testis may be at the root or shaft of the penis, or overlying the pubic bone [1, 5]. The left testis in this case was on the pubic bone more to the right side. It is the rarest form of ectopic testis with an incidence of 0.6% [3, 6, 7].
The cause of ectopic testis remains unclear [2]. However, theories have been put forward to explain ectopic testicular migration. Amongst the popular theories, Lockwood [8] proposed that ectopic testis occurred when a dominant pull was directed by minor gubernacular tails.
Pubopenile ectopic testis may be due to a mechanical obstruction at the level of the scrotum leading to deviation of the testis towards a zone of less resistance [1, 5].Other causes may include genitofemoral nerve defects, epididymal factors, decreased intra-abdominal pressure, asymmetric growth of the cord structures compared with the inguinal canal and hormonal abnormalities [2].
The diagnosis of pubopenile testicular ectopia is essentially clinical and done at birth but the patients may present late possibly due to ignorance or psychosocial reasons as in our case [1–3, 5, 7].
An ultrasound scan confirms the diagnosis and aid localization, while Doppler scan demonstrates testicular vascularization [2, 5].
We did ultrasound because it is cheap, available and helped rule out other clinical abdominal findings. Computerized tomography scan (CTS) is however useful for cryptorchidism with an intra-abdominal location of the testis [3]. In some cases, preoperative laparoscopies may be useful for diagnosis [9]. CTS and laparoscopy were not available, though their findings may not have changed our open approach of management which is faster and less technical.
The intraoperative finding of the left spermatic cord exiting from the left inguinal canal into the penopubic area differentiates it from transverse testicular ectopia where both cords would have exited together from the ipsilateral right deep ring [10].
Early surgical intervention is advocated because ectopic testis does not descend by itself [1, 2, 5]. The treatment of ectopic Pubopenile testis is usually elective though ours was discovered during emergency groin exploration. It is not technically challenging as the long spermatic cord makes orchidopexy relatively easy [2, 7].
The procedure is best done by an experienced surgeon who can handle associated structures/findings while sparing the delicate vas deferens with its blood supply.
The inguinal approach offered a good exposure for the evaluation of the hernia, full mobilization of the testis and its cord, and placement into the scrotum. This approach has been reported to be adequate for the treatment of ectopic testis [1, 2, 5].
CONCLUSION
Any inguinal or pubopenile mass in the presence of an empty scrotum should make the surgeon consider ectopic testis as one of the deferential diagnoses. Hernia obstruction and uncommon content like appendix are associated possibilities of ectopic testis.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no competing interest.
FUNDING
The authors did not receive any form of funding for this study.

{kind=link}
{kind=link}
{kind=link}