





Abstract
Phlebectasia is a rare condition that refers to the dilatation of any vein in the neck. It is more common in the internal jugular vein and in boys. Diagnosis of the condition is based on ultrasound with Doppler and contrast-enhanced computed tomography. Management of this condition is conservative unless there are complications that may require surgery. Here, we present two pediatric cases of internal jugular phlebectasia. The first patient was an 8-year-old boy, and the second was a 5-year-old boy. They both presented to our clinic with recurrent tonsillitis for tonsillectomy, and both were incidental findings.
INTRODUCTION
Phlebectasia is a fusiform dilatation of the vein; it affects any vein in the neck, and the most affected veins are the internal jugular vein, followed by the external jugular vein, and less frequently, superficial communicus and anterior jugular veins [1]. This condition is usually observed in children and is characterized by a challenging diagnosis. The incidence of this condition is rare [2]. The diagnosis is confirmed by contrast computed tomography (CT) or ultrasound (US) combined with Doppler flow imaging. Conservative treatment is the management protocol in the absence of deformities and complications [3], whereas surgical treatment is performed in cases of complications or for cosmetic reasons [2]. Here, we present two cases of internal jugular phlebectasia in two male pediatric patients.
Case 1
The first case involved an 8-year-old boy who presented to our clinic with recurrent tonsillitis and was booked for tonsillectomy. He had no contributive medical history. He was found to have an incidental midline neck mass during the evaluation (Fig. 1); this mass was found since the age of eight months. His parents denied any breathing or feeding difficulties. The mass increased with coughing and the valsalva maneuver. The mass was more toward to the right of the neck, and it was soft and compressible with no skin change.
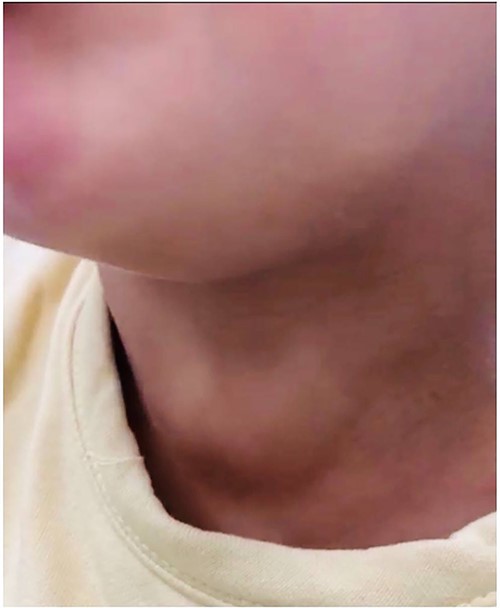
The mass on the right side of the first patient’s neck.
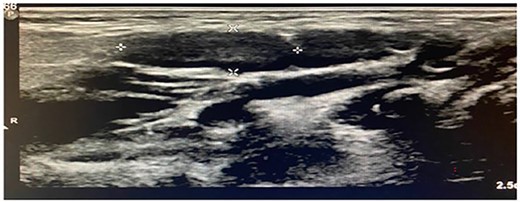
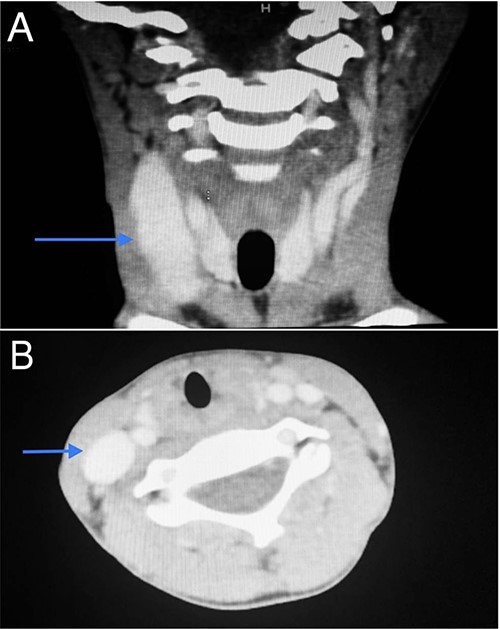
Imaging examination of the patient was done by performing CT and US. US Doppler showed a right dilated internal jugular vein (Fig. 2). The CT scan confirmed this finding, which suggested internal jugular vein phlebectasia (Fig. 3).
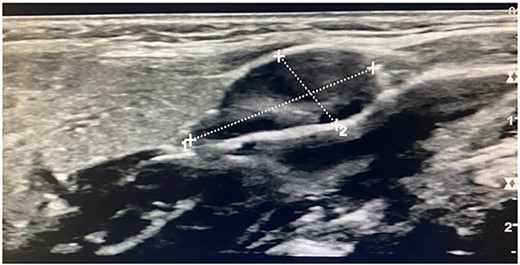
Ultrasonogram of the first patient.
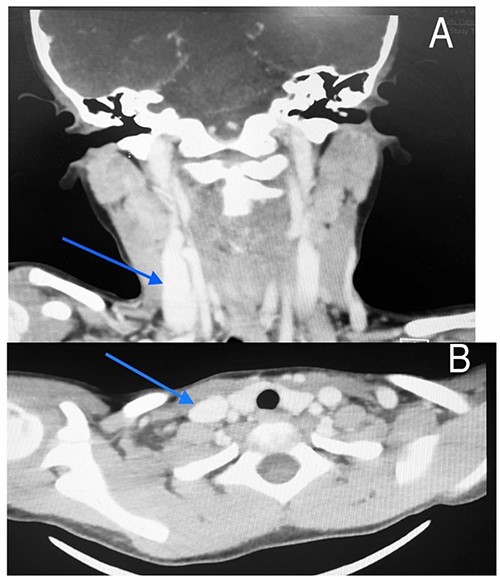
CT scan of the first patient in coronal view (A) and axial view (B) with blue indicate internal jugular phlebectasia.
Case 2
The second case involved a 5-year-old boy scheduled for tonsillectomy and was found to have a midline neck mass several years ago. The mass increased with coughing and valsalva maneuver. He had no contributive past medical history. He had no shortness of breath, dysphagia or snoring. The patient had recurrent tonsillitis and was found to have an incidental midline neck mass during the evaluation.
On examination, the midline mass was more toward to the right compressible neck mass. The mass was soft, with no skin change (Fig. 4).
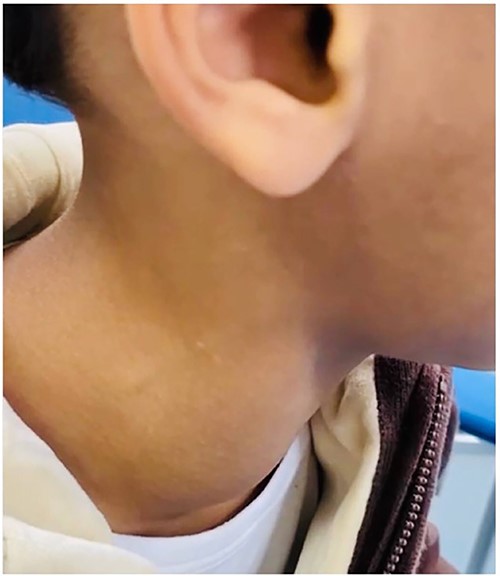
The mass on the right side of the second patient’s neck.
Imaging examination of the patient was done by performing CT with contrast and US. US Doppler showed a right dilated internal jugular vein during coughing and the valsalva maneuver (Fig. 5). CT showed a wide right internal jugular vein (Fig. 6). Both cases managed conservatively with follow-up and no surgical intervention as they did not have any complication or cosmetic concerns.
Ultrasonogram of the second patient.
CT scan of the second patient in coronal view (A) and axial view (B) with blue indicate internal jugular phlebectasia.
DISCUSSION
Jugular vein phlebectasia is also known as venous ectasia, congenital venous cyst, venous aneurysm or essential venous dilatation. Phlebectasia has been reported in all neck veins, but it appears mostly in the internal jugular vein [4]. This is a rare condition. A systematic review that included 97 articles, reported a total of 247 internal jugular phlebectasia cases in pediatric and adult patients [5]. In Saudi Arabia, only one case report of internal jugular phlebectasia in pediatric patients was reported [6]; therefore, this is the second reported case of internal jugular phlebectasia in Saudi pediatric patients.
Internal jugular vein phlebectasia is presented as a swelling in the neck, which is usually unilateral soft in consistency, and compressible; the mass increases in size during straining, such as sneezing, coughing, crying, and can be expanded by the Valsalva maneuver [4, 6]. Jugular vein phlebectasia affects children, and mostly boys than girls by twofold; it also usually affects the right side of the neck [7]. This condition was benign and asymptomatic [7].
Our cases were ideal and met all the previously reported characteristics of phlebectasia, where the patients had unilateral masses that affected the right side of the neck. The masses were found to increase during coughing and the valsalva maneuver; the masses also were found to be compressible. However, the possible differential diagnosis for swelling could be a branchial cyst, cavernous hemangioma, superior mediastinal cyst, laryngocele and cystic hygroma [8]; thus, the patients underwent Doppler US and CT with contrast to confirm the diagnosis.
Doppler US and CT with contrast are non-invasive methods for the diagnosis of Phlebectasia [4], and our patients underwent diagnostic imaging for the diagnosis and confirmation of this condition.
The possible causes of jugular vein phlebectasia include mechanical compression, vein trauma, gross anatomic abnormality, and idiopathic and congenital defects [9]. Congenital internal jugular phlebectasia corresponds to dilatation of the jugular vein with no tortuosity [10]. In our case, the patients had no stridor or airway symptoms. The patients had this for long periods without any symptoms. In addition, the patients had no previous abnormality as they were born full term through normal vaginal delivery, and were not admitted to neonatal intensive care units or had a history of trauma. This indicates that the condition was congenital or idiopathic.
The management protocol for phlebectasia is conservative treatment in the absence of deformities and complications [3], but in cases of complications or deformities, surgical treatment is performed to resolve the and for cosmetic reasons [2]. In our cases, there were no complications or deformities; therefore, they underwent conservative treatment.
CONCLUSION
Phlebectasia is a rare condition that refers to dilatation of the neck veins and affects the internal jugular vein more commonly. Internal jugular phlebectasia is more common among boys than among girls. These conditions can evolve as congenital or idiopathic defects. Our patients are the first Saudi boys with intergranular phlebectasia with no obvious reasons for phlebectasia. The patients required no treatment, as they did not have any complications or deformities.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}