





Abstract
Omental infarction is a rare cause of pain and must be considered in the differential diagnosis of acute abdomen. It arises in any quadrant that contains omentum when a compromised blood supply takes place. We report a morbid obese 45-year-old male with Diabetes mellitus, dyslipidemia and coronavirus-disease-related pneumonia 2 months prior to his emergency presentation with acute epigastric and right upper quadrant pain. The patient was investigated by computed tomography (CT), and the provisional diagnosis was biliary colic from gallbladder stone. The patient’s pain was severe and not compatible with biliary colic. Diagnostic laparoscopy approached and an incidental finding of omental necrotic area. Excision of the infarcted omentum in addition to cholecystectomy was done. The patient’s postoperative course was uneventful, and he was discharged home after 2 days. In our case, the CT image did not discover mental changes that may help us to make a preoperative diagnosis.
INTRODUCTION
Omental infarction (OI) is a rare cause of acute abdominal pain that has a presentation identical to cholecystitis, appendicitis, diverticulitis, epiploic appendagitis and mesenteric panniculitis. It is a self-limited disease without the need for surgical intervention unless the pain is severe or the diagnosis is questionable [1]. The first described case of OI was in 1896 by Bush, in a patient who presented with localized abdominal pain mainly on the right side [2].
The exact cause of OI is unknown, and some suggested redundant omentum, vascular congestion, increased intra-abdominal pressure and hyper-peristalsis due to overeating all may play a role. Risk factors such as obesity, male gender, fourth to fifth decade, trauma, heavy labor and sudden changes in body position can predispose to OI [3–6]. Although ultrasound is a specific but not sensitive tool, a computed tomography (CT) scan is considered a gold standard to diagnose OI. The management strategy should be conservative with initial pain control, failure to respond and mandate surgical intervention [4].
We reported a case of OI that presents with right upper quadrant pain mimicking biliary colic.
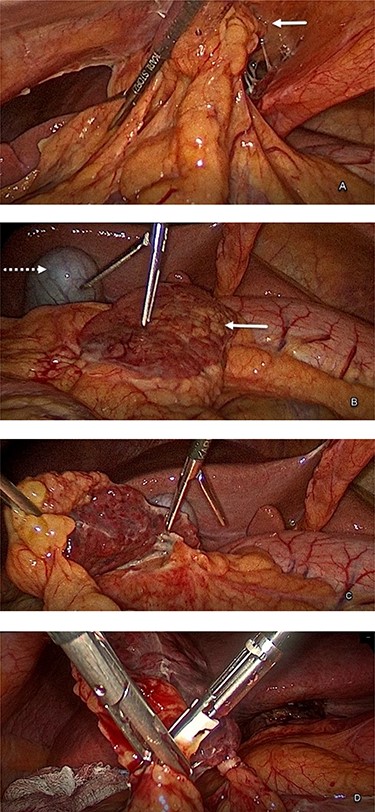
Intraoperative finding, A, the attachment of the omentum to the anterior abdominal wall. B, the white arrow indicates the demarcated dark red color omental infarction compared to the yellow color healthy omentum, and the dotted arrow indicates the gallbladder. C, dissection and excision of the omental infarction. D, excision of the infarcted part of the omentum using a bipolar device.
CASE REPORT
A 45-year-old male morbid obese class II with BMI 38, diabetic, dyslipidemic with coronavirus disease (COVID)-related pneumonia 2 months ago visited the emergency room with acute right upper quadrant pain which started suddenly with no vomiting, no jaundice, no subjective fever, no change in urine or stool color and no chest pain. Physical examination showed conscious, oriented patient with numeric pain score: 8, blood pressure 140/85, heart rate: 90, temperature: 37, respiratory rate: 19, O2 Saturation: 97%. Heart auscultation was S1 + S2 + 0, lung with equal air entry and abdomen tender right upper quadrant with no Murphy’s sign. The rest of the abdomen is soft and lax, with no rigidity.
The lab findings showed leukocyte 8.9 × 103/ul with slight high neutrophils 80%; cardiac enzymes, bilirubin, amylase, liver enzymes and albumin were within normal limits. CT abdomen and pelvis without IV contrast showed two findings: fine early fat stranding noted in the omentum anterior to hepatic flexure of the colon and 8 mm stones within the gallbladder with no sign of cholecystitis, normal appearance of all internal organ with no free air or fluid collection. The admission impression was biliary colic. The patient’s pain was not responding to pain killer on the first day of admission, and he was planned for a diagnostic laparoscopy with cholecystectomy. Laparoscopic exploration was done and intraoperative finding of necrotic part of twisted omentum attached to anterior abdominal wall at falciform ligament (Fig. 1A–D). The attachment was dissected, and the necrotic part was excised and sent to histopathology; further, cholecystectomy was done. The patient’s postoperative course went uneventful. He was discharged home on Day 2. For the last 3 months of follow-up, the patient is symptoms free and has recovered well.
Histopathology
Two specimens were sent for histopathology (Fig. 2).

The gallbladder with 8 mm stone opened inside the dish and 5 cm piece of infarcted omentum.
Gallbladder
Gallbladder consisted of specimen of measurement 8 × 3 × 0.2 cm, with smooth surface and rough mucosa consisting of chronic cholecystitis with a single stone.
Omental tissue
Omental tissue measured 5 × 3.5 × 0.5 cm, gray adipose soft tissue with a focal area of fat necrosis, fibrosis and chronic inflammation, negative for malignancy.
DISCUSSION
The greater omentum is a sizeable peritoneal fold that contains fats and blood vessels; it continues with the visceral peritoneal layers of the stomach and transverse colon. OI occurs primarily on the right side of the abdomen because the lateral edge of the omentum is freely mobile and has weakened blood supply, making it more susceptible to infarction and necrosis [5]. Reaching the accurate diagnosis of OI is unlikely, with only 5% of cases diagnosed preoperatively [6]. Pain is the most common symptom for OI in the literature; our patient presented with right upper quadrant pain, no nausea or vomiting. Studies reported a high-grade fever up to 39.5°C, which we did not record in our case. With obesity and a BMI more than 25, known as a risk factor [7], we report class II obesity with a BMI of 38. Men are twice as likely as women to have OI, which might be explained by the heavy exertion and labor nature of work done by men.
There is no definite relation between Covid 19 and OI. The COVID-19-associated coagulopathy (CAC) displays unique features that include a high risk of developing thromboembolic complications, and it may have a rule in OI [8] as seen in our report.
A diagnosis based on clinical signs alone is difficult, and most of the reported cases before 2009 were established with a laparotomy [9]. Some reports showed a trial of conservative management (Table 1).
Literature review about recent cases report of omental infarction
| Managment | Images | No. of cases | Authors | Year |
|---|---|---|---|---|
| Surgery, open | Nill | one | Paul bush | 1896 |
| Surgery, open | Nill | three | David D. Crofoot | 1980 |
| Surgery, open | US*, CT** | nine | Grattan-Smith J | 2002 |
| four conservative six surgery lap***. | US, CT | 10 | Nubi | 2009 |
| Lap. | US, CT | one | Itenberg | 2010 |
| Conservative | US, CT | one | Barai K | 2011 |
| three conservative one Lap. | US, CT | four | Park T | 2012 |
| Lap. | US, CT | five | E. S. Concannon | 2013 |
| Lap. | US | one | Smolilo D | 2015 |
| Lap. | US, CT | one | Buell K | 2017 |
| Conservative | CT | one | Udechukwu N | 2018 |
| Conservative | US, CT | one | Huai-Jie Zhang | 2020 |
| Lap. | CT | two | Tran Que Son | 2021 |
*US: ultrasound
**CT: computed tomography
***Lap; laparoscopy
Ultrasound has limited rules to diagnose OI; a CT scan can help to make the diagnosis; a pathognomonic sign is a triangular or oval-shaped fatty mass or a streaky infiltration soft tissue [10]. Our patient’s scan without contrast showed early fat stranding noted in the omentum anterior to hepatic flexure of the colon but did not accurately reach the diagnosis, which could be either due to lack of contrast or early OI.
There was a case reported in 2015 that discovered OI intraoperative, and the patient had positive Murphy’s sign [6]. The choice of management remains controversial and should be individualized depending on patient pain severity, diagnosis certainty and response to initial conservative measures. Once diagnosed preoperatively, initial pain control and conservative management should be started. Nonetheless, the infarcted omentum may undergo necrosis with progressive fibrosis that results in prolonged pain, fever and long hospital stay, and may end with abdominal abscess. So, conservative treatment is an appropriate first line of treatment for the first 24–48 h. If it fails, then laparoscopic excision of infarcted omentum should be performed without delay to decrease pain and shorten hospital stay, as well as to avoid complications [11–14].
CONCLUSIONS
OI must be considered in the differential diagnosis of acute upper abdominal pain. The management remains controversial and should be individualized, with laparoscopic exploration and infarction excision indicated in a patient with severe pain, diagnosis uncertainty and failure to responding to initial conservative measures.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}