





Abstract
Caecal volvulus represents an uncommon acute surgical presentation of bowel obstruction. Familiarity with particular long-term symptoms and pre-disposing factors can help a clinician identify caecal volvulus as a possible diagnosis. There has been a changing vogue of radiological investigation and surgical interventions. We present a summary of these options.
INTRODUCTION
Caecal volvulus is rare form of bowel obstruction, caused by twisting of the caecum, terminal ileum and occasionally the ascending colon. Given its uncommon clinical presentation, a high index of suspicion is required to prevent diagnostic and treatment delay.
CASE DESCRIPTION
A 47-year-old female patient with no significant medical comorbidities, presented with a 24-hour history of right-sided lower abdominal pain and distension. The two-year background history was suggestive of mobile caecum syndrome with episodic abdominal pain and intermittent self-resolving obstructive symptoms.
Surgical history included a laparoscopic gastric sleeve converted two years later to a Roux-en-Y gastric bypass and hiatus hernia repair. Following gastric bypass, a revision of jejuno-jejunostomy was performed due to inability to progress with diet. An appendicectomy for incidentally noted appendiceal mucocele was performed at the same time. Notably, no lateral mobilization of the caecum was performed during any of these surgical procedures.
Admission blood tests were unremarkable. Abdominal X-ray showed non-specific signs of large bowel obstruction (Fig. 1). Computed tomography (CT) scan indicated unusual location of the caecum in the right upper quadrant along with gross distension up to 13 cm (Fig. 2), a whirling pattern of mesenteric vessels (Fig. 3) and a competent ileo-caecal valve. In context of her surgical history, these findings raised concern for a closed loop obstruction due to internal herniation.

Abdominal X-Ray—right upper quadrant distended colonic loop.
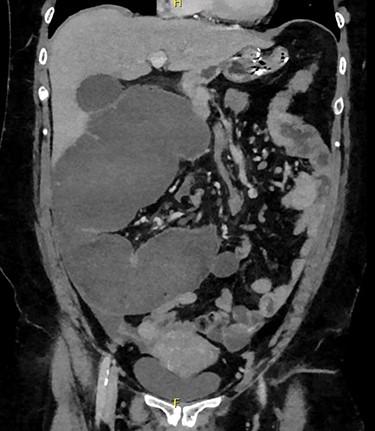
CT—distended loop of caecum in the right upper quadrant.
The patient proceeded to an emergency exploratory laparotomy on the basis of clinical and imaging findings.
Intra-operative findings were a mobile caecum with a 720° anticlockwise axial volvulus (Fig. 4). The caecum, though grossly distended, was non-ischemic without perforation. A limited right hemicolectomy with stapled side-to-side anastomosis was undertaken.
The patient had an uncomplicated recovery with a four-day hospital stay. On five-month review, the pre-operative bowel symptoms of recurrent pain and constipation had resolved.
Histology showed a limited right hemicolectomy specimen with submucosal edema and congestion consistent with volvulus.
DISCUSSION
Caecal volvulus is an uncommon cause of bowel obstruction, with an annual incidence of 1.5% of all adult bowel obstruction and accounts for 25–40% of any volvulus of the colon [1].
There are two types of caecal volvulus: organoaxial and bascule. Organoaxial caecal volvulus is the abnormal axial rotation of the caecum, usually in the clockwise direction [2]. The resultant twisting of the mesentery results in both luminal obstruction and decreased perfusion.
Caecal bascule only accounts for <10% of all cases of caecal volvulus and involves the folding of the caecum anteriorly over the ascending colon [3]. Given there is less mesenteric rotation, it is less associated with vascular compromise [3].
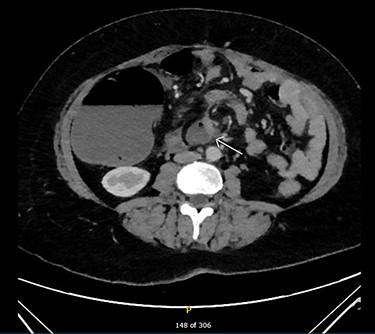
CT—mesenteric whirling (arrow).

Intra-operative picture: 720 degree axial caecal volvulus with caecal distension.
The etiology of caecal volvulus is multifactorial, with a link between congenital susceptibility and acquired risk factors.
Congenital propensity for caecal hypermobility occurs due to incomplete intestinal rotation during weeks 5–11 of fetal life. This in turn leads to abnormal fixation to the posterior abdominal wall of the right hemicolon and caecum during embryogenesis [4].
About, 20–50% of patients presenting with caecal volvulus have also had previous abdominal surgery [1]. The theory being that post-surgical adhesions provide a fulcrum increasing the risk of torsion of the hyper-mobile caecum [1, 5].
Late term pregnancy is another risk factor, as the caecum is displaced by the enlarging uterus, its mesentery elongating and increasing the propensity to twist [5].
Other acquired risk factors such as chronic constipation, adynamic ileus or severe acute medical illnesses are thought to be linked through gut dysmotility and subsequent caecal distension, this increased load can cause volvulus of the proximal colon [1, 4].
Mobile caecum syndrome is a frequent precursor to fulminant caecal volvulus, with 50% of patients reporting long-term symptoms of pain, abdominal distension and constipation [1]. Partial volvulus and peristalsis against the volved bowel causes right lower quadrant pain [4].
In terms of diagnostic imaging, computed tomography (CT) is the preferred form of radiologic examination for caecal volvulus as it is more specific for diagnosis of volvulus.
On CT several particular features are diagnostic for caecal volvulus. The ‘bird’s beak’ sign shows the tapering of proximal and distal portions of bowels progressing towards the point of torsion [6, 7]. However, the most sensitive sign is a particular ‘whirl’ that is characteristic of mesenteric torsion and engorgement of blood vessels around a fixed point [8]. Evidence of this ‘whirl’ along with direction of the twist was 93% sensitive in the determination of caecal compared to sigmoid volvulus [8].
The management of caecal volvulus requires surgical intervention. Procedures may be resectional or non-resectional. Non-resectional procedures include de-torsion, caecopexy or tube caecostomy—the insertion of tube within the lumen of the caecum that prevents twisting [1, 5, 9]. These procedures were historically popular due to relatively low mortality rates; however, high recurrence rates of 13–70% make them unfavorable now [1, 9].
Currently, the most common surgical intervention is resectional, making up 89% of all cases taken to theatre [5]. Right hemicolectomy involves colonic resection effectively eliminating any risk of recurrence [9]. Historically, emergent resectional procedures were associated with higher mortality rates, up to 39%, due to the longer operative times and increased physiological insult [1]. However, advances in perioperative care and more rapid recognition of cases due to a high index of suspicion and early use of CT imaging for diagnosis have meant the mortality rate has significantly decreased to 6.67% [1, 5].
CONCLUSION
Caecal volvulus, as a rare cause of colonic obstruction, presents a diagnostic challenge with an associated high mortality if allowed to progress to fulminant obstruction. A high index of suspicion is needed when facing a patient with apparent bowel obstruction and a background suggestive of mobile caecum syndrome. Rapid assessment with cross-sectional imaging to aid diagnosis can help make an early decision for surgical intervention. Resectional procedures are now preferred due to low recurrence and non-inferior mortality rate.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
References
Bains L, Gupta A, Kaur D, Batish A. Mobile right colon syndrome: obscure cause of lower right abdominal pain.

{kind=link}
{kind=link}
{kind=link}
{kind=link}