





Abstract
The anomalous position of nonrecurrent laryngeal nerve (NRLN) predisposes it to injury during thyroid surgery. The presence of right aberrant subclavian artery is a strong indicator of having an NRLN. Here, we are presenting a case report of an NRLN and role of imaging in its prediction.
INTRODUCTION
The nonrecurrent laryngeal nerve (NRLN) is a rare anomaly of the recurrent laryngeal nerve (RLN). NRLN directly originates from the vagus nerve in the neck without descending into the thoracic region [1]. An NRLN on the right side is consistently associated with an aberrant right subclavian artery.
CASE REPORT
We present a case report of a 47-year-old female patient with a newly detected papillary thyroid carcinoma. Her clinical examination was unremarkable, except for an asymmetrically enlarged thyroid gland, left lobe larger than the right. There was no extrathyroid or retrosternal extension or suspicious lymph nodes. She was euthyroid and her vocal cords showed normal mobility. Preoperative chest radiograph (Fig. 1) was normal.

Chest X-ray (PA view)—no mediastinal widening, normal study. PA, posteroanterior.
A preoperative magnetic resonance imaging (MRI) of the neck (Fig. 2) showed enlarged left lobe of thyroid with a solid nodule of 3.1 × 3.0 × 2.3 cm with mild mass effect on trachea. In addition, an aberrant right subclavian artery, taking a retro-esophageal, retro-tracheal course to the right upper limb was detected.
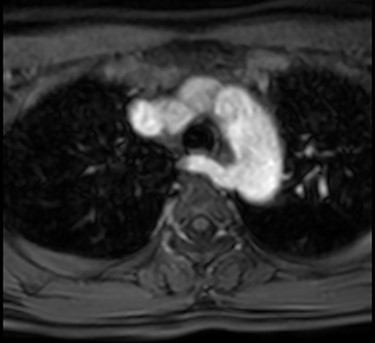
MRI with contrast showing right aberrant subclavian artery taking turn behind the trachea and esophagus.
Total thyroidectomy was carried out using intraoperative nerve monitoring with the Medtronic NIM-NEURO 3.0® nerve integrity monitoring system. During dissection, left side RLN was identified in the usual way in the tracheoesophageal groove. On the right side, an NRLN was identified (Fig. 3). It was arising from the right vagus nerve at the level of first tracheal ring, and then ascended upwards and anteriorly to the laryngeal entry point at the right cricothyroid joint. The branches of the inferior thyroid artery were seen to course superficial to the nerve (NRLN type 2b) [1] (Fig. 4). The course of the nerve in the neck was almost perpendicular to the tracheoesophageal groove rather than parallel to it. This nerve was identified at the entry point and was dissected retrograde and preserved in continuity.
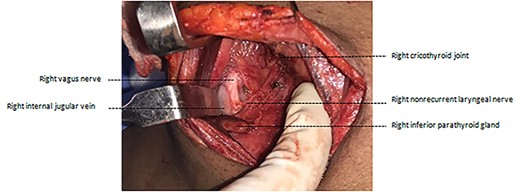
Intraoperative photograph after ligation of branches of the inferior thyroid artery.
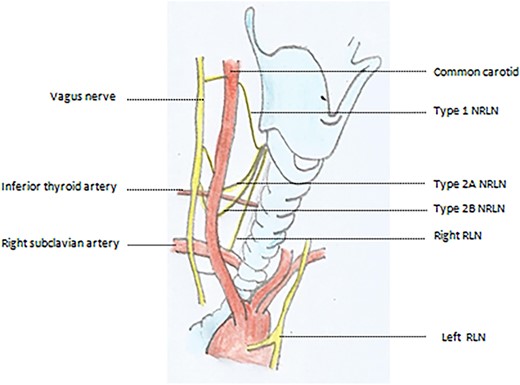
Types of NRLN with respect to inferior thyroid artery.
DISCUSSION
NRLN is a rare developmental anomaly usually associated with vascular malformation with incidence rate of 0.3–0.8% on right side and 0.004% on left side in the general population [1]. Left NRLN is always associated with situs inversus [1]. On the right side, the NRLN results from partial regression of the fourth pharyngeal arch, resulting in an aberrant subclavian artery that runs behind the esophagus. This vascular anomaly permits the nerve to migrate freely into the neck as the fetus grows longitudinally [2]. The presence of an aberrant origin of the right subclavian artery may predict an NRLN in majority of cases.
The presence of NRLN increases the risk of nerve injury during thyroidectomy. The RLN is not seen on any preoperative imaging, and hence neither is the NRLN visualized on imaging. Therefore, the detection of an arteria lusoria is a surrogate indicator of having NRLN. Chest radiograph has a low accuracy in detecting this vascular anomaly and is not a reliable method for predicting NRLN. Although barium swallow study performed for the evaluation of dysphagia lusoria will pick up this aberrant vessel; however, this is not a recommended investigation for all patients undergoing thyroidectomy. Preoperative computed tomography (CT) and MRI with or without angiograms can confirm the vascular abnormality and predict the possibility of an NRLN. However, these are not routinely recommended and feasible for all patients undergoing thyroidectomy. Hence, the NRLN is often an intraoperative ‘surprise’ finding or at times not identified or at times inadvertently injured.
Ultrasound is a simple, noninvasive and cost-effective method to screen patients scheduled for thyroid surgery for the risk of NRLN. Using an echo probe in the suprasternal notch to see the origin of subclavian artery, to look for the presence of innominate artery will help to rule out the possibility of an aberrant vessel and thus predict a right-sided NRLN reliably. ‘Y’ sign denotes the presence of the division of the brachiocephalic artery into the right common carotid artery and right subclavian artery [3]. Absence of ‘Y’ sign indicates aberrant origin of a subclavian artery.
Although this is not routinely done while performing a thyroid ultrasound, including this in the preoperative workup of a thyroidectomy will serve as a good screening tool to rule out the possibility of an NRLN and also help identify cases where a preoperative MRI/CT may be warranted, even though the primary tumor or nodal disease may not warrant the same. Such an evaluation is noninvasive and would prove to be cost effective as well when used only as a screening tool for patients scheduled for thyroid or parathyroid surgery instead of using it for routine evaluations.
CONCLUSION
We recommend a routine ultrasound and Doppler screening for vascular anomalies prior to thyroidectomy. The absence of Y-sign can help to decide which patients need a preoperative MRI/CT scan, especially where the primary or nodal disease does not warrant a scan.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}