





Abstract
Glucocorticoids are commonly used in the management of patients with brain Tumour for reducing peritumoral and vasogenic edema. However, they may lead to development of limb and life-threatening conditions such as necrotizing fasciitis (NF). NF is a rare but potentially lethal condition. Early detection and aggressive treatment may lead to decreased mortality and limb salvage. The diagnosis is predominately clinical but may be supported by laboratory and radiological investigations. Chronic steroid use not only predisposes to the development of NF but also may mask early features delaying presentation and diagnosis. Clinicians should have a high index of suspicion especially in patients on chronic steroid therapy as this may aid in early detection and treatment. We present a case report of a successful limb salvage that exemplifies these points.
INTRODUCTION
Glucocorticoids remain an important part of the armamentarium of neurosurgeons and neurologists in the management of patients with brain tumour. It is used widely for reducing peritumoral and vasogenic edema, having an important effect on quality of life. However, it may result in various adverse effects, ranging from very mild to fulminant life-threatening conditions. Steroids have an immunosuppressive effect and one of the risks of long-term use is an increased risk of (particularly bacterial) infection. Additionally, the use of steroid can mask clinical signs of florid infection leading to delayed presentation and management.
We present a case of a female patient with brain tumors maintained on dexamethasone who subsequently developed fulminant necrotizing fasciitis (NF) to the hand.
CASE
A 65-years-old right-hand dominant woman presented to our unit with a 24-h history of a progressively worsening discoloration and swelling to her left index finger (LIF) associated with generalized swelling and tenderness of the left hand. She denied any recent trauma to her left hand. She gave a history of epilepsy due to multiple meningiomas for which she was maintained on dexamethasone treatment (4 mg/day) for 6 months.
Clinical examination revealed an afebrile, relatively well-looking woman, with classic cushingnoid appearance and a grossly normal neurological examination. Gross swelling to her left hand, most markedly to the LIF, was noted. Her LIF was cold, insensate and dusky with epidermolysis of the dorsal skin (Fig. 1). She also had ascending cellulitis extending to her elbow and palpable lymph nodes on her axilla. X-ray demonstrated gross soft tissue swelling but was otherwise unremarkable, with no signs of gas within the tissues. A clinical diagnosis of fulminant NF was made; she was admitted and empirically commenced on intravenous penicillin and booked emergently for debridement of her left hand. Her laboratory analysis revealed elevated C-reactive protein 560 mg/L and white blood cell count 24 × 109U/L and hyponatremia 128 mmol/L with a LRINEC score of 7.

Images showing 65-year-old woman with initial features of NF to left hand; (A) radial view, (B and C) dorsal view, (D) volar view.
Intraoperatively, the clinical diagnosis of NF was confirmed with circumferential necrosis of her LIF. The LIF was amputated at the metacarpophalangeal joint (Fig. 2) and radical debridement was performed of nonviable skin and subcutaneous tissue on the dorsum of her left hand and distal forearm. The volar tissues and the proximal forearm demonstrated healthy bleeding skin and normal looking fascia. Postoperatively, she was managed in our high dependency unit for close monitoring. A second washout was performed 24 h later not revealing any further signs of infection. Microbiology cultures later revealed penicillin sensitive Streptococcus pyogenes species. Her wounds were resurfaced with a split thickness skin graft 2 days later (Fig. 3). She was subsequently discharged on Day 7 post presentation.
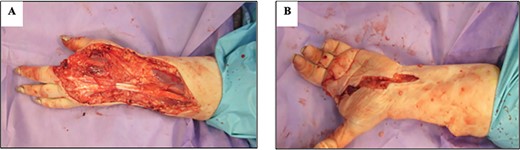
Image showing intraoperative findings post wound excision and amputation of LIF; (A) dorsal view (B) volar view.
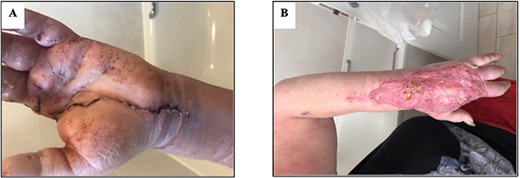
Images showing successfully salvage limb 6 weeks postoperatively; (A) volar view, (B) dorsal view.
DISCUSSION
Glucocorticoids are commonly used in the treatment of patients with brain tumour especially with symptomatic pertumoral and vasogenic edema [1]. Their implementation reduces the production of peritumor edema, thereby decreasing the potential for development of raised intracranial pressure and its potential sequelae [2].
There has been much debate regarding the optimal dose to effectively treat edema with Galicich et al. [3] suggesting maximum of 16 mg/day. Other authors have expressed concerns and suggested giving the smallest effective dose for the shortest duration to minimize side effects, which can involve significant morbidity [4].
NF is a rare but potentially lethal condition. It presents as a rapidly progressive necrotizing infection of the fascia and subcutaneous tissues. Early diagnosis and treatment is critical in reducing morbidity and mortality.
The diagnosis of NF is a clinical one, though laboratory and radiological investigations may occasionally play an adjunctive role. NF may be classified on the basis of microbiology [5] and is characterized histologically by an extensive acute inflammatory reaction, suppuration and angiothrombosis, culminating in extensive tissue necrosis [6].
Scoring systems such as the LRINEC score [7] have been proven to be a useful tool, particularly in early presentations. Patients with cumulative score > 6 have a positive predictive value of 92.0% and negative predictive value of 96.0% of NF.
However confounding factors such as chronic steroid therapy may make this tool difficult to interpret, as steroids are known to significantly affect the immune system leading to a decreased inflammatory response. Furthermore, steroid treatment may independently affect the parameters the LRINEC score creating a diagnostic conundrum.
A computed tomography (CT) scan may also play a diagnostic role in some cases [8]. However, while the LRINEC tool and a CT scan may be helpful in certain circumstances, the diagnosis of NF is primarily clinical and investigations must not delay emergency surgical treatment, as it is only early aggressive debridement that reduces mortality in these patients (in conjunction with appropriate antibiotic therapy).
Typical clinical features of NF include the rapid development of florid signs of infection, the skin may be obviously necrotic, but may simply appear red and warm in the early stages of infection. Of note, the skin often loses its turgor, in contrast with the shiny swollen appearance seen in cellulitis. Pain and, later, systemic toxicity are usually disproportionate to the cutaneous appearances. Interestingly, disproportionate pain was not a feature in our index case, which we postulate may have been due to the steroids masking some of the early clinical features.
In situations where a diagnostic uncertainty remains, the patient should be taken to operating theater and an exploratory incision can be made. The presence of brown, so called ‘dishwater fluid’ and an ability to easily sweep the skin and subcutaneous tissues off the fascia with a finger (‘finger sweep test’) confirm the diagnosis. If the skin bleeds normally and the fascia looks healthy, samples may be taken for urgent microbiology and the patient carefully monitored. Surgical exploration remains the gold standard for definitive diagnosis [9, 10].
We attribute the ‘successful’ outcome of this case to a high index of clinical suspicion resulting in early detection followed by radical debridement. The diagnosis of NF remains largely clinical and clinicians should have a high index of suspicion, especially in patients on chronic steroid therapy.
ACKNOWLEDGEMENT
None.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}