





Abstract
Intussusception of the appendix is a rare disease that constitutes a diagnostic challenge to the surgeon. Intussusception is defined as the telescoping of a segment of the gastrointestinal tract into an adjacent one. We are reporting a case of a 14-year-old boy who presented in our institution with the features of acute appendicitis. On exploration appendiculo-cecal intussusception was found for which right hemicolectomy with ileotransverse colon anastomosis was done.
INTRODUCTION
Intussusception of the appendix is a rare disease that constitutes a diagnostic challenge to the surgeon [1]. Intussusception is defined as the telescoping of a segment of the gastrointestinal tract into an adjacent one. It is the leading cause of intestinal obstruction in children and ranks second only to appendicitis [2]. The exact mechanism that precipitates intussusception is still unknown, but it is generally believed that any lesion in the bowel wall or irritant within the bowel lumen may alter the normal peristaltic pattern and is capable of starting an invagination leading to intussusception [3]. Presentation varies from acute and progressive, mimicking acute appendicitis, to chronic and protracted with intermittent symptoms. With more frequent use of computed tomography (CT) in the evaluation of patients with abdominal pain, the condition can be diagnosed more reliably. The definitive treatment for appendicular intussusception is surgical ranging from simple appendectomy to right hemicolectomy. This paper reports a case of appendiculo-cecal intussusception in a child.
CASE REPORT
A 14-year-old boy presented to our institute with a chief complaint of pain in the right lower abdomen for 1 day which was progressive, around the umbilicus which later on localized to the right iliac fossa. It was associated with multiple episodes of non-bilious vomiting. On examination, the abdomen was distended with tenderness over the right iliac fossa over McBurney’s point. Digital rectal examination did not reveal any significant findings. Laboratory parameters were within normal limits including arterial blood gas analysis report. Ultrasonography of the abdomen revealed bowel within bowel loop appearance, showing classical ‘doughnut sign’ with few prominent mesenteric lymph nodes. X-ray abdomen erect and supine films were inconclusive. The diagnosis of intussusception was made and was planned for exploration. On exploration there was intussusception of the appendix into the cecum just below the ileocecal junction (Fig. 1a). Our attempts to reduce intussusception failed due to dense adhesion, so enterotomy was done and the appendix was visualized (Fig. 1b) which was fibrosed, so right hemicolectomy was done. Postoperative period was uneventful. Histopathology findings were suggestive of appendicitis, ileitis and colitis. However, inflammatory bowel disease was not ruled out. On regular follow-up, the patient was tolerating oral diets and passing stool and flatus. Wound was healthy.
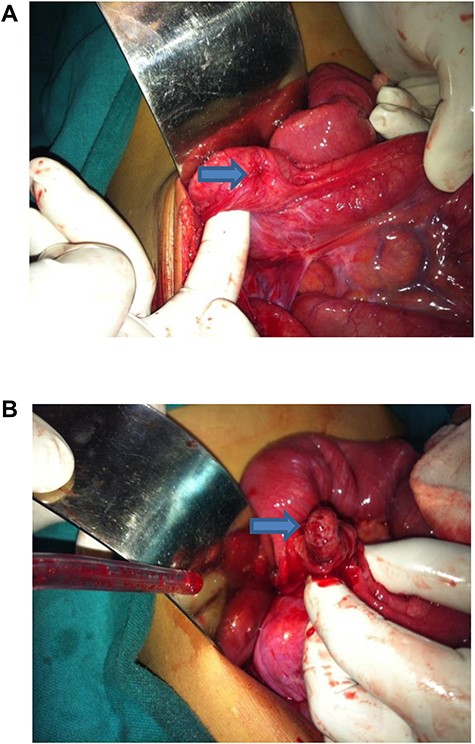
(a) Appendiculo-cecal intussusception. (b) Fibrosed appendix seen after enterotomy.
DISCUSSION
Intussusception was first reported in 1674 by Barbette of Amsterdam. In 1789, John Hunter gave a detailed report about intussusception, or introsusception. Sir Jonathan Hutchinson was the first to successfully operate on a child with intussusception in 1871 [4].
Intussusception of the appendix may occur at any age; however, majority of the reported cases reviewed in the earlier literature occurred in the pediatric age group, with an average of 16 years of age. The condition is four to five times common among the males than in the females [5]. The classic pediatric presentation of intussusception is abdominal pain and mass and blood per rectum. Other findings are fever, constipation, diarrhea, bleeding and abdominal distention. Common physical findings include abdominal distention, decreased or absent bowel sounds, guaiac-positive stool and abdominal mass [4]. Several imaging techniques may help to precisely identify the causative lesion preoperatively. Plain abdominal X-ray is typically the first diagnostic tool. Contrast studies can help to identify the site and cause of the intussusception, particularly in more chronic cases. Upper gastrointestinal series may show ‘stacked coin’ or ‘coiled spring’ appearance [6]. Barium enema examination may be useful in patients with colonic or ileocolic intussusception in which a cup-shaped filling defect is a characteristic finding. Ultrasonography has been used to evaluate suspected intussusception. The classic features include the target and doughnut sign on transverse view and the pseudokidney sign in the longitudinal view. The characteristic feature of computed tomography (CT) scan includes a target mass enveloped with eccentrically located areas of low density. Later a layering effect occurs as a result of longitudinal compression and venous congestion of the intussusception [7].
There is no universal approach to the treatment of adult intussusception. Most authors agree that laparotomy is mandatory, based on the likelihood of an underlying pathologic lesion. There has been controversy associated with the option of preliminary reduction of the intussusception before resection vs. primary resection without reduction. The theoretic objections to reduction of grossly viable bowel with mucosal necrosis are (1) intraluminal seeding and venous embolization of malignant cells in the region of ulcerated mucosa, (2) possible perforation during manipulation and (3) increased risk of anastomotic complications in the face of edematous and inflamed bowel. Reduction should not be attempted if there are signs of bowel ischemia or inflammation. Based on a high incidence of an underlying malignancy, which may be difficult to confirm intraoperatively, many authors recommend primary resection whenever possible. For colonic intussusception, most recent reports recommend a selective approach to resection, keeping in mind that the site of intussusception tends to correlate with the lesion being benign or malignant [4].
CONCLUSION
Appendiculo-cecal intussusception is a very rare entity. In children it can be managed conservatively provided there are no features of obstruction or strangulation but if features are present needs exploration.
Conflict of interest
None.
FUNDING
None.

{kind=link}