





Abstract
Odontoid fractures constitute the commonest cervical spinal fracture in the elderly. There are varied management approaches with paucity of robust evidence to guide decision-making. We review the case of a 92-years-old man with traumatic Grauer type II B odontoid fracture treated with anterior cannulated screw fixation. Postoperatively, he was noted to have dysphagia due to a zenker’s diverticulum. Further history revealed repair of a zenker’s diverticulum ~40 years prior. Cervical spine images and video fluoroscopy demonstrated a recurrent zenker’s diverticulum. After re-excision of the recurrent zenker’s diverticulum his dysphagia resolved. This unique case describes dysphagia due to recurrent zenker’s diverticulum presenting after anterior cannulated screw fixation for type II B odontoid fracture. The dysphagia was diagnosed and treated in close collaboration with speech and language therapists and otorhinolaryngologist. This underscores the importance of holistic approach to the elderly patient with odontoid fractures.
INTRODUCTION
Odontoid fractures constitute the commonest cervical spinal fracture in the elderly population [1]. Early mobilization is essential to prevent clinical deterioration from medical comorbidities or other illnesses due to prolonged recumbence with reported 16% 30-day mortality rate [2]. This has led to a more aggressive posture towards surgical stabilization of unstable type II fractures according to the Anderson and D’Alonzo classification and may be achieved by either an anterior or posterior approach [3]. The halo vest or semi-rigid cervical collar can offer equivalent and satisfactory non-operative outcomes, however the higher complication rate associated with the former makes it a less attractive choice among the elderly population. Anterior cannulated screw fixation (ACSF) affords adequate osteosynthesis and early pain control thereby allowing for the targeted early mobilization and discharge [4].
The posterior cervical instrumented fusion (PCIF) has the drawback of sacrificing the C1-C2 rotatory function and therefore temporary posterior instrumentation without fusion (PWIF) has been evaluated with promising results [5]. We review a case of a nonagenarian man with Grauer type II B odontoid fracture who was treated with ACSF by the complex spine unit at the institution [6]. Dysphagia, a common complication followed surgery however this time it was from a rather uncommon cause.
CASE REPORT
A 92-years-old man was immediately brought to the emergency department with complaints of neck pain following a fall down a flight of stairs at home. He had no comorbid illnesses and was neurologically intact. Imaging confirmed isolated type II odontoid fracture for which he had ACSF the following day. Postoperatively, he experienced dysphagia and further history revealed that he had repair of a zenker’s diverticulum ~40 years prior. A small lump was palpable in the left cervical region at the site of a previous surgical scar. Speech and language therapist, otorhinolaryngologist (ORL) and the geriatric teams were consulted while he was fed with liquid diet via a fine bore feeding tube. Preoperative cervical spine images (Fig. 1) as well as video fluoroscopy performed pre- and post-re-excision of recurrent zenker’s diverticulum (Fig. 2) are shown.

Preoperative lateral plain cervical radiograph (left), mid-sagittal (middle) and coronal (right) CT scans showing Grauer type IIB odontoid fracture without exaggeration of the atlantodental interval (ADI) suggestive of an intact transverse atantal ligament (TAL).
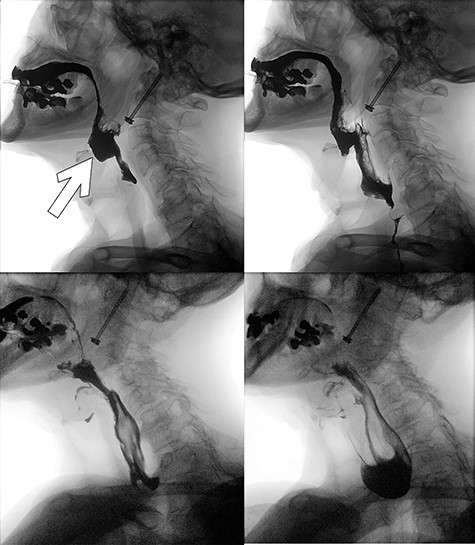
Postoperative video fluoroscopy demonstrating recurrent zenker’s diverticulum (white arrow) filling preferentially (superior left) and contrast subsequently flowing relatively easily into the esophagus following re-excision of the pouch with an incision into the cricopharyngeous muscle (inferior left and right).
His dysphagia resolved following this second operation.
DISCUSSION
Conservative versus surgical management of type II odontoid fractures in the elderly
Without clinical symptoms such as pain, signs such as weakness or radiological evidence of instability despite bony nonunion, fibrous non-union should be considered an acceptable outcome and could be followed conservatively [7]. Such non-operative management may be achieved using a cervical collar. Despite no difference in failure rate in a recent systematic review, the halo has largely fallen out of favor owing to its greater propensity for respiratory complications in potentially and already frail geriatric patients.
This nonagenarian was of good health prior to his injury however prolonged immobilization could have led to rapid physiological deterioration given his age. Early ambulation was incumbent on optimal pain control and since the cervical collar still allows for ~10° of flexion–extension at C1/C2, it was foreseeable that this approach would prove problematic [1]. As such, the decision for operative fixation was made despite an intact transverse atlantal ligament (TAL) and <6 mm distraction of fracture fragment.
Anterior cannulated screw fixation versus PCIF
Anderson and D’Alonzo Type II is further subclassified into Grauer type II A, II B and II C accounting for non-displaced, displaced transverse or anterior superior to posterior inferior and comminuted or anterior inferior to posterior superior fractures respectively [6]. Having decided upon surgery, the next dilemma was whether to stabilize from anteriorly or whether to employ a posterior approach. Given that the fracture line was from anterior superior to posterior inferior and did not involve the superior articular process of C2 (Grauer type II B), there was adequate room for purchase of the lag screw without distracting the fracture fragment as opposed to a Grauer type II C fracture [4].
Having exposed the C2-C3 intervertebral disc space, it is the practice of the institutions’ complex spine unit to use a trimmed 5 ml syringe as a working port rather than self-retaining retractors. This minimized the retraction on the adjacent soft tissue, such as the recurrent laryngeal nerve and the esophagus. This simple technique is akin to a tubular retractor but importantly, it neither required special additional equipment nor did it exert retaining pressure on the adjacent tissue that could cause neuropraxia or excite an inflammatory response with resultant edema manifesting as dysphagia.
Post-op dysphagia
Despite the added precaution outlined, the patient developed dysphagia postoperatively. At 92 years old, he was almost certain to experience dysphagia even without the recurrent diverticulum given the reported 80% risk and incremental 12% increase for each additional year beyond 65 years old (odds ratio = 1.12, 95% Confidence Interval: 1.001, 1.258) [8].
We identified 30 cases of zenker’s diverticulum formation after anterior cervical surgery but not in case of ACSF for Odontoid fracture [9, 10]. Whilst dysphagia was a recognized complication following ACSF. This report is to the best of our knowledge, the first of this nature.
Holistic management of geriatric patients with type II Odontoid fractures
The authors concede that involving the geriatric team from admission could have elucidated the patient’s dietary modification prior to hospitalization however this short-coming did not lead to prolonged hospitalization or harm in any way [1]. This underscores the importance of holistic approach to the elderly patient with odontoid fracture.
Anterior cannulated screw fixation is the preferred technique for type II B Odontoid fractures in the elderly patient. It is a quick and safe, motion preserving technique to stabilize these fractures. Dysphagia following ACSF is a common complication, which is usually transient. However, this is the first reported case of dysphagia due to recurrent zenker’s diverticulum presenting after ACSF for type II odontoid fracture. The dysphagia resolved following excision of the zenker’s diverticulum.
ACKNOWLEDGMENTS
We would like to thank Mr. Aprajay Golash, Mr. Carl Bruce, Mr. Mark Morgan, Dr. Dwight Webster, Professor Ivor Crandon and Professor Renn Holness for insightful management guidance and manuscript reviews.
Conflict of interest statement
The authors declare that there are no conflict of interest and that the work herein was not funded by grant or any other contributions from funding agencies.
Funding
The authors hereby declare that this work has not been supported by grants or other forms of contributions from funding bodies.

{kind=link}
{kind=link}